
Clinical Skills
ocd
i-cbt

Stay in the loop
Trauma-informed tools, new trainings, and the occasional pep talk. No spam, ever.

Read Time:
A trauma therapist is mid-session with a young adult client when the client's phone buzzes. The client glances at it, types a quick response, and returns to the conversation. The therapist notices but does not interrupt. Over the next few sessions, she observes the same pattern. The phone buzzes. The client checks. A few words. Back to therapy. By the third session, the client mentions, almost in passing, that her mother sends her a text every two hours during the workday to confirm she is safe. The mother has been doing this since the client was a teenager. The client does not love it, but she has learned that not responding produces a level of escalation in the household that is not worth the cost. So she responds.
The therapist is sitting with a piece of family accommodation. The mother is not unwell. The mother is loving and engaged and worried. And yet a behavior that began as care has become, over a decade, a structural feature of the family system. The client cannot quite tell the therapist what the texts are for. The mother probably could not either, if asked directly. The pattern has become its own logic.
This is family accommodation, and in OCD-impacted clients it does significant clinical work. It maintains the disorder. It shapes the family system around symptom management. It quietly undermines treatment in ways that can be hard to see from inside the therapy room. And for trauma therapists whose clients have comorbid OCD, family accommodation is one of the most common reasons treatment that should be moving forward stalls between sessions.
This piece is about what family accommodation is, why it matters for trauma work, the SPACE program developed to address it, and how to talk to families about it in a way that does not produce shame.
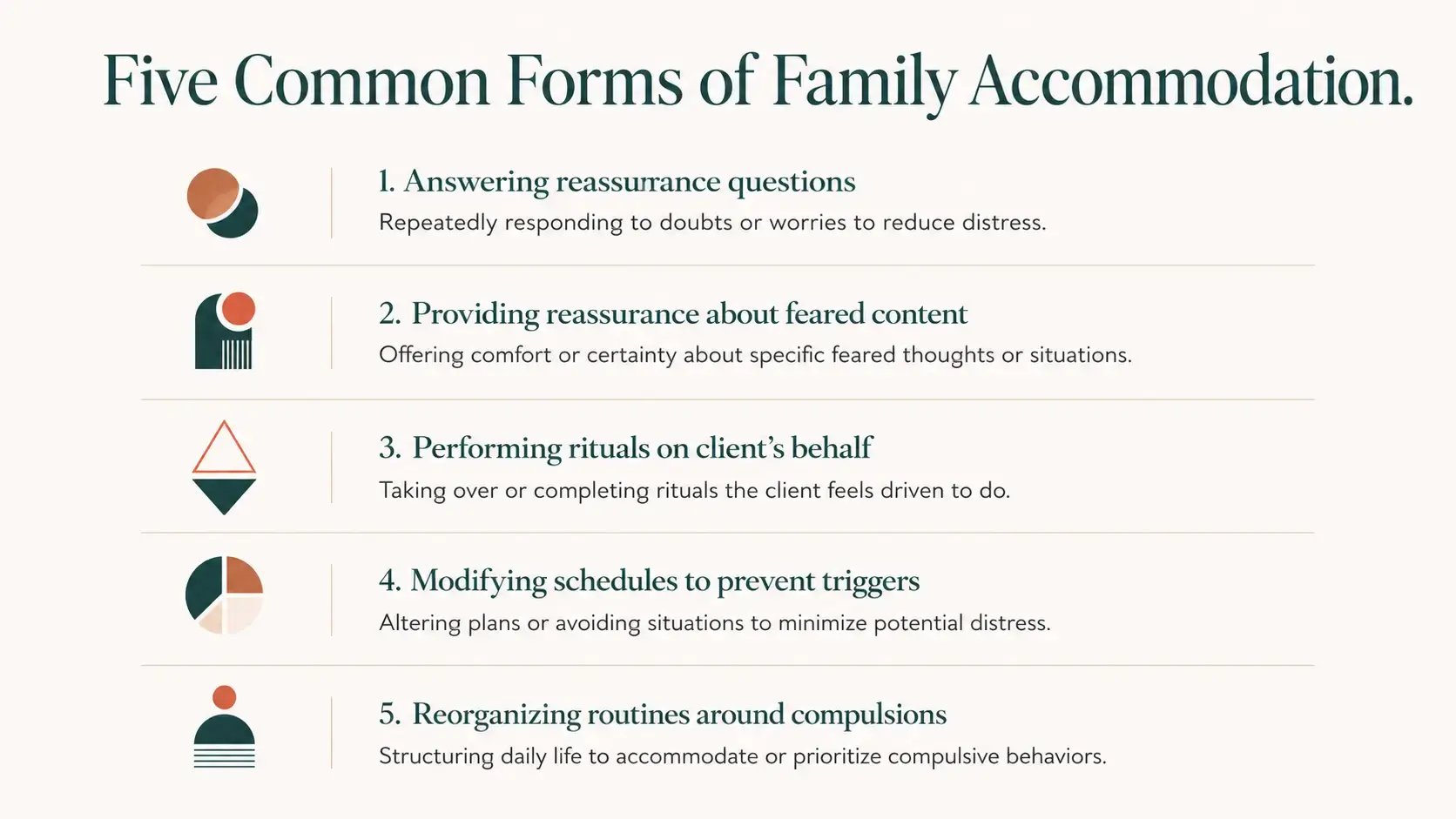
Family accommodation refers to the ways family members modify their own behavior to reduce a client's distress, prevent a feared outcome, or participate directly in compulsive rituals. The accommodation can take many forms: answering reassurance questions, providing reassurance about specific feared content, performing rituals on the client's behalf, modifying schedules to prevent triggering situations, avoiding topics that produce distress, or reorganizing household routines around the client's compulsive system.
The most rigorous recent synthesis is Hermida-Barros and colleagues (2024), an updated systematic review and meta-analysis of family accommodation in OCD that drew from 76 studies and concluded that accommodation is highly prevalent across both pediatric and adult OCD populations, with the majority of families showing some level of accommodation behavior.
The same review found a consistent relationship between accommodation severity and OCD symptom severity: families who accommodate more have clients with more severe symptoms.
The causal direction is not simple. Severe OCD generates strong family pressure to accommodate. Accommodation, in turn, maintains the OCD by removing the natural consequences of compulsive behavior and preventing the corrective experiences that might otherwise reduce obsessional anxiety. The two reinforce each other across time, and family systems with OCD-impacted members often arrive at a steady state in which accommodation has become invisible to everyone involved because it has been going on for years.
This is not a story about bad families. The families who accommodate are, in nearly every case, families who love the client and are trying to reduce their suffering. The accommodation is, in the moment, kind. It is also, across time, one of the strongest maintaining factors for the disorder. Both things are true.
The clinical relevance is that the accommodation cannot be separated from the OCD picture. A client whose family accommodates extensively is not just a client with OCD. They are a client whose OCD is being sustained by a relational system that has organized itself around symptom management. Treatment that addresses the client without addressing the accommodation tends to produce slow, partial gains that regress between sessions. Treatment that addresses both moves more decisively.
Accommodation is often invisible to the family, but it is rarely invisible to clinical attention once the clinician knows what to look for. The patterns show up in several recognizable ways.
The first is the client's relational anxiety about practicing new behaviors at home. A client who can engage in session with a new approach, who agrees with the rationale, and who then reports that practicing at home was impossible because of how the family responded, is often describing accommodation pressure. The accommodation is so embedded that any disruption of the accommodation produces escalation, conflict, or relational rupture. The client learns to stop trying.
The second is repetitive references to specific family behaviors that the client describes as not OCD related. The mother who texts every two hours. The partner who checks the door even when they were not the last one out. The sibling who avoids certain conversation topics. The roommate who has stopped using the kitchen at certain times. These behaviors often present in the clinical conversation as quirks of the family, not as accommodation. The clinical move is to listen for them across sessions and start to map the pattern.
The third is the way the client describes their own functioning at home versus elsewhere. A client who reports doing well at work, at school, or in social settings but coming home and finding themselves unable to function is often describing a context in which the accommodation system both enables and traps them. Outside the home, they cope. Inside the home, the accommodation system absorbs the coping function, and the client's capacity narrows accordingly.
The fourth is the family's reaction to treatment progress. A client whose family responds to treatment gains with subtle resistance, with renewed anxiety about the client's wellbeing, or with new accommodating behaviors that emerge as old ones decrease, is in an accommodation system that is being threatened by the client's improvement. The family is not consciously sabotaging treatment. The system is reorganizing to maintain its homeostasis.
And the fifth is the client's own discomfort when asked to identify accommodation. Clients who have grown up inside an accommodation system often experience the suggestion that the family is accommodating as a kind of betrayal, even when they intellectually understand the clinical point. The discomfort itself is data. It often signals an attachment-laden accommodation pattern that will require careful relational work to address.
SPACE stands for Supportive Parenting for Anxious Childhood Emotions. It was developed by Eli Lebowitz at the Yale Child Study Center, and it is the most rigorously researched parent-based treatment for childhood and adolescent anxiety and OCD. SPACE works exclusively with the parents. The child or adolescent is not required to participate in treatment. The intervention targets the accommodation behaviors directly, with the parents learning to reduce accommodation while increasing supportive responses to the client's distress.
The evidence base for SPACE is substantial and growing. Multiple randomized controlled trials have demonstrated that SPACE produces outcomes comparable to direct child-focused cognitive behavioral therapy for child and adolescent anxiety, with the significant advantage that the child does not need to engage with treatment for the intervention to work. The Yale Child Study Center maintains an overview of the SPACE evidence base and clinical training pathway, and the protocol is now in widespread clinical use internationally.
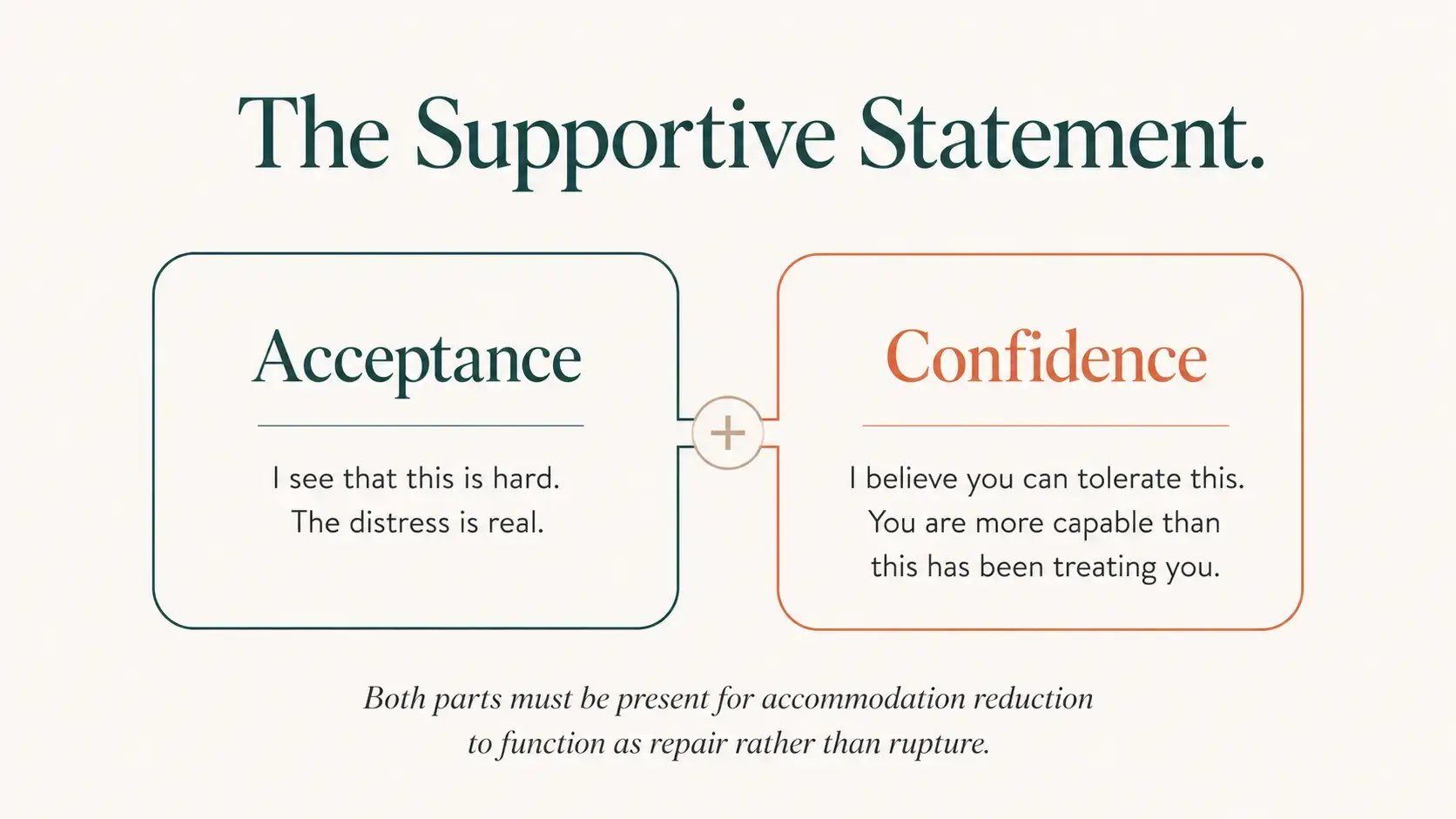
The core principle of SPACE is that accommodation reduction must be paired with what Lebowitz calls supportive statements. A parent who is reducing accommodation needs to communicate two things simultaneously to the client. The first is acceptance: the parent recognizes that the client's distress is real, that the obsessions are difficult, and that the client is not being asked to perform calmness or pretend nothing is happening. The second is confidence: the parent expresses belief that the client can tolerate the distress without the accommodation, that the client is more capable than the system has been treating them as, and that the parent is not going to abandon the relationship as the accommodation changes.
This two-part supportive statement structure is what distinguishes SPACE from simply telling parents to stop accommodating. Without the supportive frame, accommodation reduction often produces relational rupture, increased child distress, and parent guilt that pulls the system back into accommodation. With the supportive frame, accommodation reduction becomes a relational repair: the parent communicates that they love the child enough to stop performing the accommodation that has been quietly disabling them.
SPACE is delivered over a series of sessions, typically 10 to 12, with the parents identifying specific accommodation behaviors, planning gradual reductions, and developing the supportive statement language for each one. The protocol is highly structured but adaptable to family context, including divorced and blended families, single-parent households, and adult-child situations where the principles can be adapted to spouses, partners, and adult children living at home.
Trauma therapists may wonder why a body of literature developed primarily for childhood OCD belongs in a conversation about adult trauma cases. Several reasons are worth considering.
The first is that accommodation does not end at age 18. Adult clients with OCD and comorbid trauma often live inside accommodation systems that have been operating for decades. The accommodating party may be a spouse, an adult parent, a sibling, an adult child, or a roommate. The structural dynamics are the same as in childhood accommodation, even when the relational configuration is different. The clinical relevance is the same.
The second is that accommodation undermines trauma treatment between sessions. A client doing EMDR for trauma, who returns home to an accommodation system that absorbs every wave of post-session activation by performing reassurance, ritual participation, or schedule modification, is in a relational environment that is actively counteracting what the trauma work is trying to produce. The client learns, week after week, that the accommodation absorbs distress more reliably than the trauma processing does. The accommodation wins.
The third is that some trauma presentations look like OCD presentations until the accommodation is named. A client whose distress, intrusions, and avoidance appear to be primarily trauma response may, on closer examination, be operating inside an accommodation system that is shaping the clinical picture in ways the trauma framing does not capture. Naming the accommodation can clarify which condition is doing the most clinical work, and which treatment direction is most likely to produce movement.
The fourth is that accommodation can stall what looks like otherwise solid trauma work. We have written elsewhere about the relational dynamics that complicate trauma therapy when couples are involved, and the family accommodation literature extends the same insight to a wider set of relational configurations. Trauma work cannot be sealed off from the relational system the client lives inside.
And the fifth is that recognizing accommodation opens new referral options. A trauma therapist whose client is operating inside a family accommodation system can refer the accommodating family member, often the parent, sometimes the spouse, to a SPACE-trained provider for parallel work. The two treatments do not have to be done by the same clinician. They do have to be coordinated. The trauma work moves more decisively when the accommodation pattern is being addressed in parallel.
The accommodation conversation is one of the most relationally delicate in OCD treatment. Done well, it produces relief, clarity, and motivation. Done poorly, it produces defensiveness, family rupture, and disengagement from treatment. Several principles are worth holding.
The first is to start with the function of the accommodation, not the behavior. "It sounds like you have been doing something that is, in some moment, the most caring thing available to do. You have been responding to your child's distress in the way that reduces it fastest, and you have probably been doing it for years. That makes sense." The accommodation is named as care first, even before it is named as accommodation.
The second is to name the cost of the accommodation in the client's own language. The accommodation has been keeping the OCD alive. The accommodation has been preventing the corrective experiences the client needs to develop tolerance for distress. The accommodation has been narrowing the client's life by removing the situations that would otherwise generate growth. The cost is structural, not personal.
The third is to make clear that accommodation reduction is not punishment. The parent is not being asked to be cold. The parent is being asked to do something harder: to communicate love through trust rather than through accommodation. This is the most counterintuitive part of the conversation for many families, and it is also the most clinically central.
The fourth is to introduce the supportive statement language directly. "What it looks like to reduce accommodation is to say, when your child asks the same question for the fourth time, something like this: I love you. I see that this is hard. I trust that you can tolerate not knowing the answer to this question right now. I am not going to answer it again, because answering it has been part of what is keeping it active. And I am here." The script makes the abstract concrete.
The fifth is to anticipate the escalation that often follows. Accommodation reduction commonly produces a temporary increase in the client's distress and demand for accommodation. This is the system testing whether the change will hold. Families need to be prepared for this in advance, with specific plans for how to maintain the new posture during the testing period.
And the sixth is to refer when appropriate. A trauma therapist who is not SPACE-trained and is sitting with a complex accommodation system has done good clinical work by naming the pattern, beginning the conversation, and referring the accommodating party to a provider with the specific training. The trauma work continues. The accommodation work happens in parallel. The system has more support.
Can SPACE work for adults? Yes. The original protocol was developed for parents of children and adolescents, but adapted SPACE protocols are now used with parents of adult children, spouses, partners, and other accommodating family members. The structural principles are the same. The supportive statement language adapts to the relational configuration.
What if the accommodating family member refuses to engage? The accommodation persists, and the treatment plan needs to account for it. The trauma work may still proceed, but with realistic expectations about what is workable given the relational system. Naming the accommodation with the client, even when the family member is not participating in treatment, often gives the client more agency to recognize and disrupt accommodation patterns as they emerge.
Is accommodation reduction safe for clients with comorbid trauma? Yes, with attention to pacing. Aggressive accommodation reduction in a client with significant trauma history can produce destabilization, particularly if the accommodation has been functioning as a regulation strategy for trauma-driven distress. Gradual reduction, paired with strong supportive statements and parallel trauma work, is usually the safer pathway.
Do I need to be SPACE-certified to use any of this? No. SPACE certification is required to deliver the full protocol, but knowing the model, recognizing accommodation patterns, and referring to SPACE-trained providers is meaningful clinical use. The trauma therapist who can name the pattern and refer well has expanded what is available to her clients far beyond what undifferentiated OCD referral provides.
Many of the cases that have stalled inside accommodation systems start to move once the accommodation is recognized. Not always quickly. Not always dramatically. But the work begins to have somewhere to go. The client experiences the clinical conversation differently. The family, if they are open to it, begins to consider their own role in the system without taking on guilt that would only produce more accommodation. The trauma work proceeds with a context that supports it rather than absorbs it.
Family accommodation is one of the underrecognized maintaining factors for OCD in adult and adolescent caseloads. For trauma therapists, recognizing it is not about becoming a family therapist. It is about adding a clinical literacy that changes what can be seen, named, and addressed. The work moves again. Sometimes it moves for the first time.
OCD Treatment Overview for Trauma Therapists: A 1-Day OCD and PTSD Comorbidity Training is a live training with Bronwyn Shroyer, LCSW, a co-founder of OCD Training School and one of the first Inference-based CBT trainers in the world. The training includes a working overview of family accommodation patterns and the SPACE program, alongside the differential diagnosis, evidence-based treatment, and clinical decision-making content trauma therapists need to recognize OCD in their caseloads. 6 CEs (ACE, NBCC, APA). Live September 17, 2026, with on-demand access after.
I Want a Framework for OCD and Trauma Together →
Hermida-Barros, L., Primé-Tous, M., García-Delgar, B., Forcadell, E., Lera-Miguel, S., de la Cruz, L. F., Mataix-Cols, D., & Fullana, M. A. (2024). Family accommodation in obsessive-compulsive disorder: An updated systematic review and meta-analysis. Neuroscience & Biobehavioral Reviews, 162, 105678. https://www.sciencedirect.com/science/article/pii/S0149763424001787
Kartal, F., Polat, H., & Kurt, A. (2025). Investigation of the relationship between family accommodation, alexithymia, and emotional regulation difficulty in obsessive-compulsive disorder. Psychiatry Investigation, 22(12), 1368-1378. https://pubmed.ncbi.nlm.nih.gov/41382346/
Lebowitz, E. R., Marin, C., Martino, A., Shimshoni, Y., & Silverman, W. K. (2020). Parent-based treatment as efficacious as cognitive-behavioral therapy for childhood anxiety: A randomized noninferiority study of supportive parenting for anxious childhood emotions. Journal of the American Academy of Child & Adolescent Psychiatry, 59(3), 362-372. https://pubmed.ncbi.nlm.nih.gov/31265874/
