
When Couples Therapy and Trauma Therapy Collide: Clinical Decision-Making in the Room
Apr 02, 2026
Reading Time: 10 minutes
Written By: The TTI Team
You are twenty minutes into a session. One partner just brushed against something. You could see it happen in real time: the slight shift in posture, the way their eyes went somewhere else, the SUD climbing before they could stop it. Their partner, sitting three feet away, clocked all of it. Arms crossed now. Jaw tight. Already building a wall.
And you are sitting there holding three things at once: the protocol you were trained in, the relational frame you are trying to maintain, and the very live question of what to do in the next thirty seconds.
This is not a scenario covered in EMDR Basic Training. It is not covered in standard couples therapy coursework either. And yet here you are, in it, having to make a real clinical decision right now.
That gap, the space between trauma therapist training and actual EMDR clinical decision-making in a dyadic context, is what this post is about. Not theory. Not a checklist you print out and laminate. A real framework for the moments when both worlds activate at once and you have to navigate without a map.
The Training Gap Nobody Talks About
Here is something most therapists doing this work will privately admit: they pieced together their approach to conjoint EMDR through trial and error. Maybe some expensive post-graduate supervision. Maybe a single seminar that helped. Mostly, though, through sitting in sessions that did not go the way they expected and figuring it out afterward.
This is a structural problem.
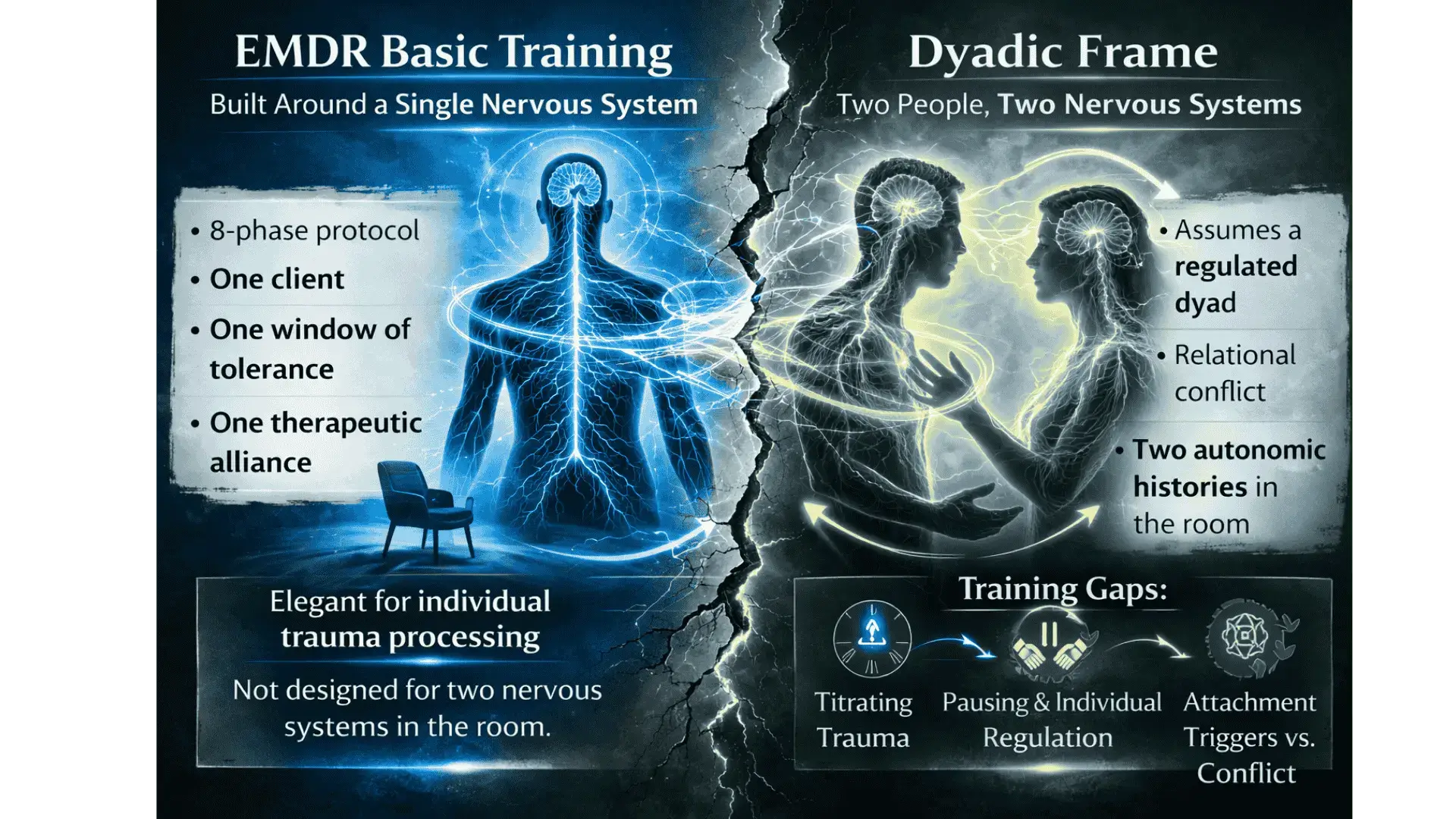
EMDR Basic Training is built around a single nervous system. The 8-phase protocol assumes one client, one window of tolerance, one therapeutic alliance to manage. It is a remarkably elegant system for individual work. But it was not designed for the moment when a second person is in the room, watching the first person activate, and bringing their own autonomic history to that observation.
Standard couples therapy training has a different blind spot. It assumes a reasonably regulated dyad working through relational conflict. It does not cover how to titrate trauma processing within a dyadic frame, when to pause relational work to address individual dysregulation, or how attachment triggers can look exactly like present-moment conflict when they are actually something much older.
A 2022 thematic analysis on integrating EMDR and EFT in couples therapy found that even therapists trained in both models described significant challenges bringing them together in practice. Not beginner therapists. Trained, experienced clinicians who still felt the seams between the two approaches in the room.
Most therapists either overcorrect or under-correct. They over-structure, running individual EMDR segments with the partner sitting silently like an observer in a fishbowl. Or they under-correct, pushing relational processing when one or both partners are not regulated enough to access it. Neither is wrong exactly. Both are attempts to solve a problem nobody adequately trained you for.
The good news is that EMDR clinical decision-making in the couples context is a learnable skill. It just requires a different framework than the one you were given.
Reading the Room: When to Stop the Reprocessing
This is the question TTI hears most from therapists doing this work. "How do I know when to pause? How do I know when to not even start?" The answer is not in the 8-phase protocol because it depends on variables that only exist in the couples room.
Here are the clearest clinical indicators. Stop reprocessing, or do not start, when:
- The observing partner is visibly dysregulated. Crossed arms, flat affect, escalating tension, withdrawal. A dysregulated witness is not a neutral presence. Their nervous system is actively in the room, influencing the processing environment whether or not they say a single word.
- The activation is relational, not memorial. If the SUD is rising because of something their partner just did, that is a couples issue first. Trying to run an EMDR protocol on a present-moment relational trigger is trying to use the wrong tool. It will stall, and it may make things worse.
- You cannot close the session safely in the time remaining. Incomplete EMDR session management in an individual frame is already complex. In a couples frame, you have two people who need to drive home together and co-regulate (or fail to) until next week. That is a significantly higher closure bar.
- There are signs of dissociation without an established partner response plan. If dual awareness is slipping and there is no clear protocol for how the observing partner responds to that, pausing is not a clinical failure. It is the right call. Research on structural dissociation and EMDR stabilization is clear that containment comes before processing, always.
A practical three-question check, run it fast when you feel the session shifting:
The research on factors influencing EMDR processing quality documents something most clinicians already sense: the variables that affect processing outcomes are often more nuanced than formal research captures. Clinician judgment, relational context, and session-level attunement matter enormously. You already knew that. Now you have permission to act on it.
Two Nervous Systems, One Room: Managing Mismatched Windows of Tolerance
In individual EMDR, monitoring the window of tolerance is a single-channel task. You are tracking one person. In couples work, you are tracking two autonomous nervous systems that are also influencing each other in real time. This is not a metaphor. It is interpersonal neurobiology.
A partner in sympathetic activation can pull the other person out of their window without anyone saying a word. A flooding partner is not just a distraction. They are an active input. And because the therapeutic relationship is triadic, the therapist's own nervous system is also in the room, functioning either as a third co-regulatory anchor or as an additional source of dysregulation if the therapist is anxious and trying to manage too many variables at once.
So the question becomes: how do you manage two different window-of-tolerance levels in couples therapy when those levels are not just different but actively affecting each other? Here is the honest answer: you cannot always bring both partners into their window simultaneously using the same intervention. One may need grounding for hypo-arousal. One may need paced breathing or containment for hyperarousal. You are running two parallel stabilization tracks while also holding the relational frame.
Understanding the window of tolerance as a relational phenomenon, not just an individual one, changes how you approach the entire session structure. Polyvagal theory supports this: as Porges's research on the science of safety makes clear, co-regulation is a biological process, not a therapeutic nicety. Nervous systems respond to each other. That is the context in which you are working.
Three practical strategies that address this directly:
- Dyadic resourcing before any reprocessing work. Both partners resource, not just the identified client. This is not a warm-up. It is a structural intervention that establishes a shared regulated baseline before anything activating begins.
- Explicit autonomic check-ins at session opening. Normalize this as part of the structure. "Before we get into anything today, I want to take thirty seconds and check in with both of you. Just notice where you are landing right now." This is not an interruption. It is the session.
- Window-of-tolerance contracts established early in treatment. Both partners know their own signals. Both know what the therapist will do when those signals appear. This removes the ambiguity and the shame from the moment of pause. It is not failure when the session slows down. It is the plan working.
For a deeper clinical grounding in the window of tolerance as applied to trauma and couples work, the NICABM framework is worth reviewing. The TTI Polyvagal-Informed EMDR course also addresses the dyadic application of these concepts in significant depth.
When One Partner Floods: What to Do in the Next 60 Seconds

This is the scenario that produces the most clinician freeze. One person is actively flooding. Sympathetic hyperarousal, above the window, not going to be able to do any meaningful relational or processing work right now. The other partner is watching. And you have a split second to decide who to orient to and how.
First: flooding during a couples session is not a therapeutic failure. It is a physiological event. Having an established response plan for it, and having communicated that plan in advance, is the difference between a session rupture and a corrective relational experience.
The most common error therapists make in this moment is attending exclusively to the flooding partner while the observing partner's experience becomes invisible. But the observing partner has just watched their person dysregulate in front of them. That is either activating their own history or confirming their worst fears about what couples therapy is going to ask of them. Both need acknowledgment. Neither can wait until next week.
Here is a sequencing that works:
- Name the physiological state without pathologizing it. You are not diagnosing. You are providing polyvagal psychoeducation in real time. "What I am noticing is that your system has moved into a protective response right now. That makes complete sense given what we just touched. Let's slow everything down."
- Slow the pace of the session, not just the person. Everything drops: the rate of speech, the density of intervention, the expectation of insight. The session is now about regulation, and that is enough.
- Use the stop signal or containment exercise established in Phase 2. The EMDR Phase 2 stabilization work exists precisely for this. If it was not established, add it to the case formulation now.
- Brief orienting acknowledgment to the observing partner. "I want to make sure I come back to you in a moment and hear how that landed." This is not perfunctory. It prevents their experience from calcifying into resentment or withdrawal while you are attending to their partner.
- Once regulated, decision fork: return to relational work or close the session. The structure of EMDR therapy is explicit that sessions should not end with a client still in a destabilized state. In couples work, that applies to both people in the room.
The research on EFT and EMDR integration highlights de-escalation as a prerequisite for any meaningful trauma or relational work. That is not a soft principle. It is the clinical sequence.
A Framework for In-Session Decision-Making (Not Just a Checklist)
Checklists break down in the couples context because the variables are too dynamic. What works is building an internalized decision framework: a set of questions the therapist can run quickly when faced with an unexpected clinical moment. Something more like a compass than a script.
The difference between following the EMDR protocol and real clinical decision-making in couples therapy is exactly this: the protocol assumes a controlled environment. Clinical decision-making accounts for the environment you are actually in. You need both. They are not in competition. But in the couples room, judgment has to precede protocol.
Here is a three-axis model that experienced clinicians tend to run, even if they have never named it that way: 
The research on multi-directed partiality in couples therapy makes clear that the therapist's ability to maintain fairness and hold both partners' perspectives simultaneously is not just a therapeutic nicety. It is a structural requirement for the work to hold. And as noted in research on therapeutic neutrality in couples therapy, neutrality in the strict sense is not really achievable or even desirable. What matters is equitable attention, deliberate and visible.
The University of Guelph thesis on multi-directed partiality and therapeutic alliance in couples and family therapy offers a useful deep dive if this dimension of the work is unfamiliar. Most therapists underweight it when one partner is in acute distress. That is exactly when it matters most.
Why Specialized Training Changes Everything
Go back to the opening scenario. One partner is activated. The other is shutting down. You have thirty seconds and two nervous systems and a therapeutic alliance to maintain.
Now imagine running that same moment with an internalized three-axis framework instead of a protocol that was never designed for this configuration. You already know your first move: check the window of tolerance, both people. You already know your second: is this memory-driven or relational? You already know how to name the physiological state without pathologizing it, how to acknowledge the observing partner, how to use what was established in Phase 2. The session does not go perfectly. But it does not rupture either.
That is not talent. That is training.
The clinical wisdom required to navigate EMDR couples therapy well has historically been locked behind expensive supervision, post-graduate certifications, and years of hard-won trial and error. That transmission model works, eventually, for therapists who can access it. But it is not the only path, and it is not equally available to everyone.
Dr. Grace Chen's EMDR with Couples course was built for exactly the moment described at the top of this post. Not for the theory of it, but for the live clinical reality of two nervous systems, one room, and a therapist who needs a map. The course addresses Phase 1 and 2 in the couples context, the decision framework for when to proceed versus pause, how to manage mismatched windows of tolerance, and what to do when one partner floods and the session needs to find its footing.
The TTI EMDR Basic Training gives you the protocol foundation. This course gives you what comes after: the clinical judgment to use it well in the room.
The Training Gap Is Real. And It Is Fixable.
The clinical anxiety that comes from not having a framework for these moments is real. It is not a reflection of your competence. It is a training gap. The therapist who freezes when both partners activate simultaneously is not a bad clinician. They are working without a map in territory that requires one.
The EMDR clinical decision-making framework covered in this post is not exhaustive. It is a starting point. The full clinical development happens in training, in practice, in supervision, and in sessions that do not go the way you planned and teach you something because of it.
But having a framework changes the experience of those moments from anxiety-producing to navigable. That shift, from freeze to orient, is what good trauma therapist training actually produces.
If the scenarios in this post feel familiar, and if the gap between your EMDR training and your couples work has been producing clinical stress you have been managing on your own, this course is the next step.
Ready to build a real clinical framework for EMDR in the couples room? Learn more about Dr. Grace Chen's EMDR with Couples course and get the training that takes you there.
References
Linder, J. N., et al. (2022). Thematic analysis: Integrating EMDR and EFT in couple therapy. PMC9544644. https://pmc.ncbi.nlm.nih.gov/articles/PMC9544644/
Porges, S. W. (2022). Polyvagal theory: A science of safety. PMC9128615. https://pmc.ncbi.nlm.nih.gov/articles/PMC9128615/
Shapiro, F. (2014). The role of EMDR therapy in medicine. PMC3951033. https://pmc.ncbi.nlm.nih.gov/articles/PMC3951033/
Faretta, E., et al. (2021). The structure of EMDR therapy. PMC8185342. https://pmc.ncbi.nlm.nih.gov/articles/PMC8185342/
PMC FLASH of Hope (2021). EMDR incomplete sessions and closure. PMC7839656. https://pmc.ncbi.nlm.nih.gov/articles/PMC7839656/
Shapiro, F. (2012). EMDR conceptual framework: Phase 2 and stabilization. PMC3122545. https://pmc.ncbi.nlm.nih.gov/articles/PMC3122545/
Factors influencing quality of processing in EMDR therapy (2024). PMC11403636. https://pmc.ncbi.nlm.nih.gov/articles/PMC11403636/
Structural dissociation and EMDR (2017). PMC5632787. https://pmc.ncbi.nlm.nih.gov/articles/PMC5632787/
Siegel, D. J. Window of tolerance. Psychology Tools. https://www.psychologytools.com/resource/window-of-tolerance
Multidirected partiality in couples therapy (2025). PMC11786296. https://pmc.ncbi.nlm.nih.gov/articles/PMC11786296/
Therapeutic neutrality in couples therapy (2024). PubMed 38424739. https://pubmed.ncbi.nlm.nih.gov/38424739/
University of Guelph thesis: Multidirected partiality and therapeutic alliance in CFT. https://atrium.lib.uoguelph.ca/xmlui/handle/10214/8356
Stay connected with fun info, news, promotions and updates!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.



