Somatic EMDR Training: How to Safely Bring the Body Into EMDR Therapy
Mar 10, 2026
Read Time: 9 minutes
Written By: The TTI Team
When EMDR and the Body Don't Match
You know that moment. Your client just finished a set of bilateral stimulation, and you ask them what they're noticing. They look at you and say, "I'm fine. Nothing really." But their shoulders are up around their ears. Their jaws are clenched tight enough to crack a walnut. Their breath is so shallow you can barely see their chest move.
Or maybe it's the opposite. They say all the right words about feeling better, but their body has gone somewhere else entirely. Flat affect. Glazed eyes. That particular quality of "present but not really here" that you've learned to recognize in trauma work.
Here's what nobody tells you in basic EMDR training: the gap between what clients say and what their bodies are doing is where complex trauma lives. And if you don't know how to work with that gap, you're going to get stuck. A lot.
This is where somatic EMDR training becomes less of a nice-to-have and more of a "how am I supposed to do this work without it?" kind of essential. Because trauma doesn't just live in narrative memory. It lives in the clench of a fist that never got to fight back, the breath that stopped mid-inhale when the world became dangerous, the muscles that are still braced for an impact that happened years ago.
Why the Body Matters in EMDR Therapy
Let's do a quick refresher on why we're all here in the first place. EMDR's Adaptive Information Processing (AIP) model tells us that trauma gets stuck when the brain can't properly process an overwhelming experience. The memory gets stored in fragments, disconnected from the larger memory network, frozen in time with all its original intensity.
That's the theory. Here's the reality: a lot of that "stuck" information isn't stored in the parts of the brain that deal with words and coherent narratives. It's stored in implicit memory, the kind that shows up as sensation, posture, impulses, and those automatic body responses we call the threat response cycle.
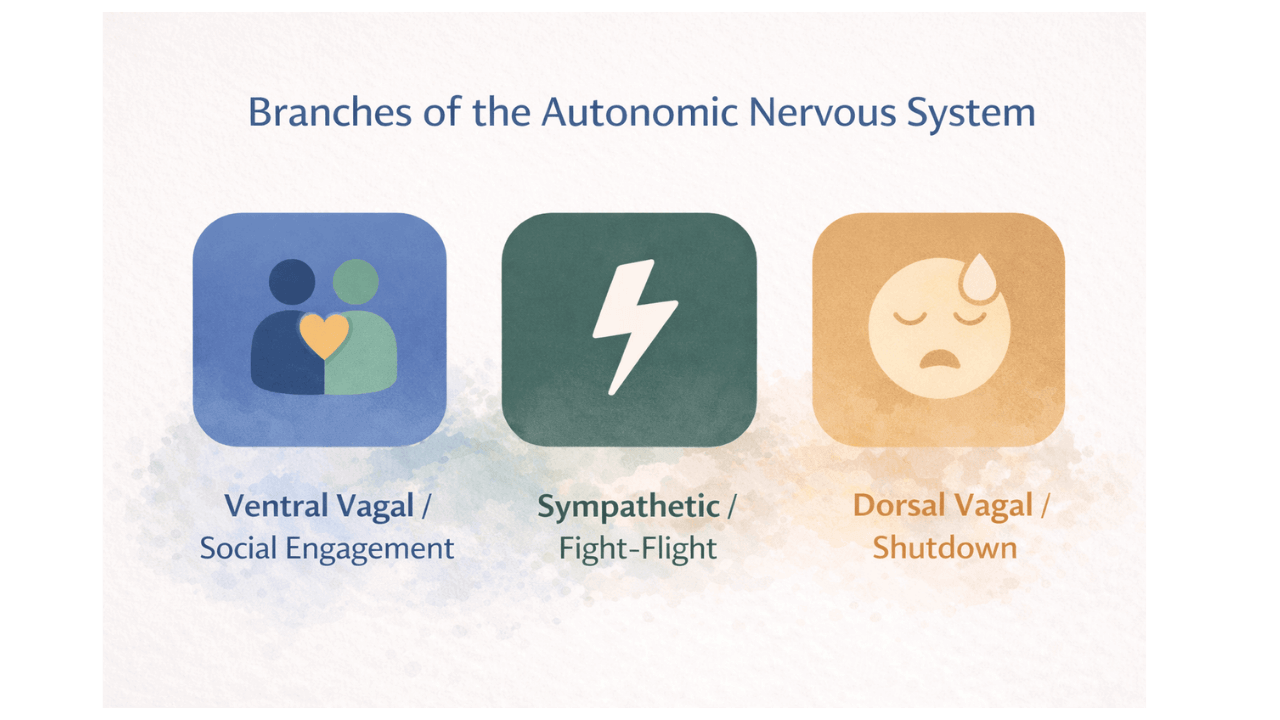
You've probably heard about polyvagal theory by now. If you haven't, the extremely simplified version is this: your nervous system is constantly scanning for safety or danger (a process called neuroception), and it responds through three main pathways. Social engagement when we feel safe. Fight or flight when we detect a threat. Shutdown and collapse when fighting or running isn't possible. These responses happen in the body before conscious awareness kicks in.
So when you're sitting with a client doing EMDR, and their body is screaming "danger!" while their words are saying "I'm okay," which one do you think is telling you the truth?
Ignoring the body in EMDR therapy leads to some predictable problems. Processing gets stuck in loops where the client keeps circling back to the same material without resolution. Or they shut down entirely, dissociate, and you lose them. Or they flood with too much activation and you spend the whole session trying to get them back into their window of tolerance instead of actually processing trauma.
None of this is because EMDR doesn't work. It's because complex trauma requires more than the standard protocol was designed to handle.
What Is Somatic EMDR? (And What It Is Not)
Here's where people get confused, so let's clear this up right away.
Somatic EMDR is not a different modality. You're not abandoning EMDR to become a somatic therapist. You're not throwing out the 8-phase protocol or pretending the AIP model doesn't exist. What is somatic EMDR, exactly? It's EMDR done with an understanding of how trauma lives in the body and how to work with that reality safely and effectively.
Think of it this way: standard EMDR training gives you a really good map for working with single-incident trauma in relatively stable clients. Somatic EMDR training gives you the tools to navigate the terrain when that map doesn't quite match what you're seeing in the room.
What somatic EMDR is NOT:
It's not turning every session into a bodywork session where you spend 45 minutes doing breathing exercises and never get to actual reprocessing. It's not cramming every somatic intervention you've ever learned into your EMDR work just because you can. It's not using "somatic" as an excuse to wing it without structure or direction.
The whole point is fidelity plus flexibility. You're staying true to the EMDR protocol while adapting your approach to meet the client's nervous system where it actually is, not where the protocol assumes it should be.
Key Somatic Skills Every EMDR Therapist Needs
Alright, let's get practical. If you're going to integrate somatic work into your EMDR practice, there are some core skills you need to develop. These aren't optional extras. They're the difference between doing EMDR safely with complex trauma and hoping for the best.
Somatic History-Taking and Case Conceptualization
Standard EMDR history-taking focuses on identifying targets and creating a treatment plan. Somatic history-taking goes deeper. You're learning to assess not just what happened, but how it lives in the body right now.
This is where concepts like the "nests of our lives" and the capabilities approach come in. You're looking at a person's entire developmental context. What resources did they have access to? What protective responses were available to them, and which ones weren't? How has trauma shaped not just their symptoms but their fundamental sense of what's possible in the world?
This kind of assessment changes everything about target selection and timing. You might discover that the client's panic attacks aren't random at all. They're happening in situations that unconsciously remind the body of times when there was no escape. Or you learn that a client who seems "resistant" to processing actually doesn't have the nervous system capacity yet to handle what processing would bring up.
When you understand the somatic landscape, you stop pushing for targets the client's system isn't ready to handle. You start working with the body's wisdom instead of against it.
Orienting and Neuroceptive Safety
Here's a scenario that happens all the time in trauma therapy: you're about to start reprocessing, and your client is already activated before you even bring up the target memory. Their body is reading the therapy room, maybe even you, as a potential threat.
Before you can do any meaningful trauma processing, you need to help the client's nervous system register that right now, in this moment, they're actually safe. This is called orienting, and it's one of the most powerful somatic interventions for EMDR therapists.
Orienting means bringing someone's attention to the present-moment environment in a way that allows their nervous system to assess safety. It's different from standard grounding techniques because you're not trying to distract from the distress. You're helping the client's body update its threat assessment.
Here's what this might sound like:
"Before we go there, I want you to take a moment and just let your eyes move around the room. Notice the windows, the light coming in, the door. You can even notice that the door is closed and we're the only ones here. What do you notice about the room right now?"
Then you wait. You watch for the small shifts. The softening in the shoulders. The breath that gets a little deeper. These are signs that the nervous system is down-regulating, moving toward a state where processing is actually possible.
Why does this matter for EMDR? Because if a client starts bilateral stimulation while their body is already in a threat state, you're not processing the target memory. You're processing the current sense of danger, and everything gets muddled together. Neuroceptive safety isn't just a nice idea. It's a prerequisite for effective trauma work.
Titration and Pendulation
If you've done any reading about somatic trauma therapy, you've probably come across these terms. They sound fancy, but the concepts are actually pretty straightforward.
Titration means working in small, manageable doses. Instead of asking a client to dive into the full intensity of a traumatic memory, you're finding the edges of the experience. Maybe you start with just the moment before the trauma happened, when there was still some sense of agency. Or you work with a less intense memory that has similar themes.
Think of it like adjusting the temperature in a bath. You don't jump into scalding water. You test it, adjust it, make sure it's something you can actually tolerate.
Pendulation is about rhythm and movement. You're not keeping someone in the hard stuff for extended periods. You're moving between discomfort and resource, between activation and settling, between past and present. This back-and-forth motion is actually how the nervous system naturally processes and integrates difficult experiences.
In EMDR for complex trauma, titration and pendulation become essential because the window of tolerance is often pretty narrow. Push too hard, too fast, and you get flooding or shutdown. Work too cautiously, and nothing moves. Finding that sweet spot where the client is challenged but not overwhelmed is the art of this work.
You're not working cliffs here. You're working edges. There's a difference.

Somatic Channels of Experience
Here's a framework that will change how you listen in session: sensation, image, affect, behavior, and meaning. These are the five channels through which we experience the world, and trauma shows up differently in each one.
Standard EMDR focuses heavily on the image (what do you see when you bring up the memory?) and the meaning (what's the negative cognition?). Somatic work adds the other channels to the conversation.
Sensation: What do you feel in your body? Where do you feel it? What's the quality of that sensation?
Image: What do you see? (This one you already know.)
Affect: What emotions are present? (This one too.)
Behavior: What does your body want to do? What impulse is there, even if you're not acting on it?
Meaning: What does this say about you, the world, the future? (Your negative and positive cognitions live here.)
Why does this matter? Because some clients can't access images or don't have clear emotional awareness. But they can feel the tightness in their chest. They can notice the impulse to push away. They can track sensation. Understanding these different channels gives you multiple entry points for processing.
It also helps you refine your negative and positive cognitions. Sometimes a client will tell you their NC is "I'm not safe," but when you track somatically, what emerges is actually "I can't protect myself" or "I have no control." The body often knows the truth before the words catch up.
Completion of Thwarted Defensive Responses
This is where somatic EMDR training gets really interesting. And honestly, it's where a lot of therapists feel like they're stepping outside their comfort zone, so let's talk about what this actually means.
When something traumatic happens, our bodies automatically try to protect us. We fight, we flee, we freeze. But in trauma, especially developmental or complex trauma, those protective responses often couldn't complete. The child who wanted to run but couldn't. The person who wanted to fight back but was overpowered. The impulse that got cut off mid-action and never finished.
That incomplete defensive response doesn't just disappear. It gets stuck in the body. You see it show up as chronic tension, as startling easily, as that feeling of always being braced for something. The nervous system is still trying to finish what it started decades ago.
In somatic EMDR, you're creating space for that completion to happen, but in titrated, safe ways. This doesn't mean you're having clients physically fight or run during session (please don't). It means you're tracking for those small impulses. The hands that want to push. The jaw that wants to clench. The legs that want to flee.
And then you're working with those impulses in Phase 4 of EMDR. Small movements. Gentle completions. "What does your body want to do right now? Can you feel that impulse? Let's just notice it. You don't have to act on it, but see if you can feel it there."
Sometimes just acknowledging the impulse is enough. Sometimes you invite small, contained movements. A pushing motion against your own hands. A "no" that the throat has been holding for years. These micro-movements can unlock processing in profound ways.
Research on trauma and the body confirms what somatic practitioners have known for years: unfinished defensive responses keep the nervous system in a state of hypervigilance. Allowing completion, even symbolically, helps the system finally let go.
Where Somatic Work Belongs in the 8 Phases of EMDR
Let's be really clear about this because it's where EMDR therapists training in somatic approaches often get confused. Somatic interventions don't replace the 8-phase protocol. They support it.
Phases 1-2 (History and Preparation): This is where somatic assessment happens. You're gathering information about how trauma lives in the body, assessing nervous system capacity, and teaching resources that include body-based regulation tools. Orienting exercises, breath work, finding places of safety or groundedness in the body - all of this belongs in Phase 2.
Phase 3 (Assessment): When you're activating the target, you're tracking the somatic channels. Not just "what image do you see?" but "what do you notice in your body?" You're checking in with the nervous system before you start bilateral stimulation. If someone is already flooded or shut down just from thinking about the memory, you're not ready to process. You need more preparation.
Phase 4 (Desensitization): This is where it all comes together. You're doing standard bilateral stimulation, but you're tracking somatically the whole time. When processing stalls, you might bring attention to sensation. When someone dissociates, you might pause and orient. When incomplete defensive responses start to emerge, you create space for small completions. The structure of EMDR doesn't change. Your awareness of what's happening in the client's body adds depth and safety to the process.
Phases 5-8 (Installation through Reevaluation): Somatic check-ins continue here. During installation, you're not just asking if the positive cognition feels true. You're asking how it feels in the body. During body scan, you're doing what the phase already asks for but with more skill and nuance. And in reevaluation, you're tracking whether the nervous system has actually integrated the changes or if the body is still holding onto patterns.
The point is this: EMDR therapy and somatic interventions aren't competing approaches. They're complementary. When you understand how to work with the body, you're making EMDR safer, more effective, and more attuned to what complex trauma actually needs.

Common Pitfalls EMDR Therapists Face When They "Go Somatic"
Now for some real talk. I've seen therapists get really excited about somatic work and then make some predictable mistakes. Let's save you some time and client confusion by naming them upfront.
Pitfall #1: Technique Overload
You just took somatic training. You learned seventeen different grounding techniques, five types of resourcing, three models of nervous system regulation, and now you're trying to use all of them in every session. Your client is drowning in interventions and has no idea what actually helps.
Here's the thing: more isn't better. Depth is better. Pick a few somatic interventions that make sense for your client's specific needs and nervous system, and get really good at those. Master orienting before you add pendulation. Get comfortable with titration before you start working with defensive impulses. Build your skills one layer at a time instead of throwing everything at the wall to see what sticks.
Pitfall #2: Abandoning EMDR Structure
This one happens when therapists get so interested in the somatic content that they forget they're doing EMDR at all. Sessions turn into hour-long somatic explorations where you're tracking sensation and working with movement but never actually processing trauma targets.
Somatic awareness is a tool, not the goal. The goal is still adaptive resolution of traumatic memories. The goal is still helping clients integrate their experiences so they're not running their lives from the past. EMDR gives you a structure for getting there. Don't abandon it just because you found something interesting in the body.
Pitfall #3: Getting Lost Without Direction
Sometimes therapists start following somatic content without any clear clinical reasoning. "Oh, you feel tightness in your chest? Let's spend 20 minutes exploring that." Meanwhile, you've lost track of what target you're working on, what phase of EMDR you're in, and where this is all going.
Every somatic intervention should have a purpose. Is this helping establish safety? Is this resourcing before reprocessing? Is this allowing a defensive response to complete? Is this helping the client stay within their window of tolerance during processing? If you can't answer why you're doing what you're doing, you're wandering.
This is exactly why training and consultation matter. Learning how to integrate somatic interventions into EMDR isn't something you figure out from a blog post or a weekend workshop. It requires supervised practice, clinical feedback, and the kind of skill development that comes from actually doing this work under the guidance of someone who's been there.
How to Choose Somatic EMDR Training for Trauma Therapists
So you're convinced that you need this training. Smart. Now the question is: which one?
Not all somatic EMDR training is created equal, and honestly, the field is full of programs that either teach you somatic techniques divorced from EMDR context or teach you EMDR for complex trauma without actually understanding how the body works. You need both.
Here's what to look for:
Anchored to EMDR Fidelity and AIP
Any trauma therapist training program worth your time and money should still be grounded in the AIP model. You're not learning a totally new framework. You're learning how to apply EMDR principles when clients present with complex trauma, dissociation, and nervous system dysregulation. If a program asks you to abandon the 8 phases or implies that standard EMDR doesn't work, be skeptical.
Clear Somatic Case Conceptualization Model
You don't just need techniques. You need a way of thinking about cases that integrates both EMDR and somatic principles. How do you assess readiness for processing? How do you know when to use somatic interventions versus when to proceed with standard bilateral stimulation? A good training teaches you a framework for clinical decision-making, not just a grab-bag of cool techniques.
Practical Interventions, Not Just Theory
Theory is important. Understanding polyvagal theory, attachment theory, and the neurobiology of trauma matters. But if the training is all lecture and no practice, you're going to walk away with a lot of information and no idea how to actually use it in session. Look for programs that include demonstrations, practice opportunities, and real-world application.
Trainer With Both EMDR and Somatic Depth
This is crucial. You want someone who's not just intellectually curious about somatic work but has deep training and clinical experience in both EMDR and body-based trauma therapy. Rebecca Kase, for example, is an EMDRIA-Approved Consultant and Facilitator who's also extensively trained in polyvagal-informed and somatic approaches. That combination matters. You're learning from someone who's integrated these approaches in their own practice, not someone who's stitching together things they learned from different sources.
The reality is that EMDR training for complex trauma needs to prepare you for what actually shows up in the room. Not the straightforward PTSD cases you learned about in basic training, but the clients who dissociate mid-session, who can't access targets without flooding, who've been told they're "treatment resistant" when really they just needed someone who understood how to work with their nervous system.
Your Body Is Already in the Room
Here's what we want you to take away from all of this: the body is already in the room. It's always been there. Your clients' bodies are communicating constantly, whether you're trained to listen or not.
The shoulders that creep up when certain topics come close. The breath that shallows out. The eyes that go distant. The hands that clench. The fidgeting that intensifies. Every single one of these is information. Every single one of these is the nervous system trying to tell you something about the trauma you're working with.
The question isn't whether to bring the body into EMDR therapy. The question is whether you know how to listen to what it's already saying and how to work with what you find there safely and effectively.
Standard EMDR training gave you incredible tools for trauma processing. Somatic EMDR training gives you the skills to use those tools with the clients who need them most - the ones with complex trauma, developmental wounding, and nervous systems that don't fit neatly into the basic protocol.
You already know how to do EMDR. Now it's time to learn how to do it with the full complexity and wisdom of the body in the room.
Ready to Deepen Your EMDR Practice?
If you're looking for EMDR training that includes somatic and polyvagal interventions, training that gives you practical skills for working with complex trauma and dissociation, training that doesn't ask you to choose between EMDR fidelity and somatic depth - there's a path forward.
The Somatic EMDR Training: Advanced Trauma Therapy Practitioner Program is designed specifically for EMDR therapists who are ready to safely integrate body-based interventions into their trauma work. This isn't about learning a bunch of disconnected techniques. It's about developing a cohesive approach to EMDR for complex trauma that respects both the structure of the protocol and the wisdom of the nervous system.
You'll learn somatic history-taking and case conceptualization, how to use the body's signals during EMDR reprocessing, how to work with dissociation and nervous system regulation, and how to help clients complete the defensive responses that have been stuck for years. All of it grounded in both EMDR fidelity and evidence-based somatic principles.
Because your clients deserve a therapist who can work with the whole of their experience - not just the parts that fit neatly into the protocol you learned in basic training.
The body is already telling you what it needs. Are you ready to listen?
Note: This article is for educational purposes and does not constitute clinical advice. EMDR should only be practiced by trained and certified mental health professionals.
References
Adu-Gyamfi, K., Osei-Tutu, A., Adjorlolo, S., & Andoh-Arthur, J. (2021). Towards an African psychology of trauma: Commentary on the applicability of the polyvagal theory in an African context. Frontiers in Psychology, 12, Article 675583. https://www.frontiersin.org/articles/10.3389/fpsyg.2017.01578/full
Kase, R. (n.d.). Rebecca Kase, LCSW: EMDR therapy and trauma treatment. Rebecca Kase, LCSW. https://www.rebeccakase.com
Lee, C. W., & Cuijpers, P. (2013). A meta-analysis of the contribution of eye movements in processing emotional memories. Journal of Behavior Therapy and Experimental Psychiatry, 44(2), 231-239. https://pubmed.ncbi.nlm.nih.gov/18314305/
Schalinski, I., Elbert, T., & Schauer, M. (2011). Female dissociative responding to extreme sexual violence in a chronic crisis setting: The case of Eastern Congo. Journal of Traumatic Stress, 24(2), 235-238. https://pubmed.ncbi.nlm.nih.gov/19396540/
Shapiro, E., & Maxfield, L. (2019). The efficacy of EMDR early interventions. Journal of EMDR Practice and Research, 13(4), 291-301. https://pmc.ncbi.nlm.nih.gov/articles/PMC9012004/
Trauma Therapist Institute. (n.d.-a). Dissociation demystified: A conceptual guide for trauma clinicians. https://www.traumatherapistinstitute.com/Dissociation-Demystified-A-Conceptual-Guide-for-Trauma-Clinicians
Trauma Therapist Institute. (n.d.-b). Embodied somatic interventions for trauma healing. https://www.traumatherapistinstitute.com/Embodied-Somatic-Interventions-for-Trauma-Healing
Trauma Therapist Institute. (n.d.-c). Integrating EMDR with somatic practices: A holistic approach to trauma healing [Blog post]. https://www.traumatherapistinstitute.com/blog/Integrating-EMDR-with-Somatic-Practices-A-Holistic-Approach-to-Trauma-Healing
Trauma Therapist Institute. (n.d.-d). Integrative polyvagal training: Merging theory with therapeutic application [Blog post]. https://www.traumatherapistinstitute.com/blog/Integrative-Polyvagal-Training-Merging-Theory-with-Therapeutic-Application
Trauma Therapist Institute. (n.d.-e). Polyvagal techniques for nervous system regulation [Blog post]. https://www.traumatherapistinstitute.com/blog/Polyvagal-Techniques-for-Nervous-System-Regulation
van der Kolk, B. A., Stone, L., West, J., Rhodes, A., Emerson, D., Suvak, M., & Spinazzola, J. (2014). Yoga as an adjunctive treatment for posttraumatic stress disorder: A randomized controlled trial. Journal of Clinical Psychiatry, 75(6), e559-e565. https://pmc.ncbi.nlm.nih.gov/articles/PMC8457046/
Yehuda, R., Daskalakis, N. P., Bierer, L. M., Bader, H. N., Klengel, T., Holsboer, F., & Binder, E. B. (2016). Holocaust exposure induced intergenerational effects on FKBP5 methylation. Biological Psychiatry, 80(5), 372-380. https://pmc.ncbi.nlm.nih.gov/articles/PMC8835026/
Zhang, Y., Liu, Z., Zhang, R., Zhang, H., Yang, B., Sun, S., & Luo, Y. (2023). The neurobiological mechanisms underlying the effects of exercise interventions in autistic individuals. Frontiers in Neuroscience, 17, Article 1094688. https://pmc.ncbi.nlm.nih.gov/articles/PMC10505816/
Zhu, X., Suarez-Jimenez, B., Lazarov, A., Helpman, L., Papini, S., Lowell, A., Durosky, A., Lindquist, M. A., Markowitz, J. C., Schneier, F., Wager, T. D., & Neria, Y. (2018). Exposure-based therapy changes amygdala and hippocampus resting-state functional connectivity in patients with posttraumatic stress disorder. Depression and Anxiety, 35(10), 974-984. https://pmc.ncbi.nlm.nih.gov/articles/PMC12302812/
Stay connected with fun info, news, promotions and updates!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.