DBT Training for EMDR Therapists: Building a Skills-Based Framework for High-Risk Trauma Clients
Apr 15, 2026
When Your EMDR Caseload Is Always "On the Edge"
You know the feeling. You check your phone before a session and there is already a message. A client in crisis, a cancellation after a rough night, a voicemail that starts with "I just need to let you know I'm okay." And your body, that well-trained clinical instrument, registers all of it before you've had your coffee.
This is the texture of a high-acuity trauma caseload. Not dramatic. Not exceptional. Just relentless. And if you are doing EMDR work with complex trauma clients, you already know that the standard eight-phase model, as powerful as it is, does not always account for the chaos that lives between sessions.
Clinician exhaustion in this context is not a personal failing. It is a structural one. When your training hasn't given you a clear framework for managing chronic suicidality, ongoing self-harm, and severe emotion dysregulation alongside EMDR processing, you end up improvising your way through every crisis. That improvisation has a cost. It costs your clients predictability, and it costs you something harder to name: the quiet confidence of knowing you have the right tools for the job.
DBT training for EMDR therapists directly addresses that gap. Not by replacing what you already do well, but by giving you a scaffold. A shared language. A skills-based framework that makes the high-risk parts of trauma work feel less like a high-wire act and more like structured, phase-oriented trauma treatment.
Where EMDR Shines, and Where It Needs Support
EMDR is one of the most well-researched trauma therapies available. The evidence for its effectiveness in treating PTSD is robust, and for single-incident trauma with adequate stabilization, it can produce results that feel almost startling in their speed and depth. If you have done EMDR work with clients who were ready for it, you know the experience of watching a memory lose its charge. There is nothing quite like it.
But EMDR requires something that complex trauma clients often do not yet have: a nervous system stable enough to hold dual awareness, ride activation, and return to baseline within the window of a session. Research consistently shows that for clients presenting with severe emotion dysregulation, chronic suicidality, or repeated hospitalizations, jumping into reprocessing without adequate stabilization often leads to session derailments, increased crisis episodes, and therapeutic rupture.
Timing, as any experienced EMDR therapist will tell you, is everything. EMDRIA's own guidance on adapting the eight phases for elevated-risk clients is clear: reprocessing is contraindicated when a client's stabilization foundation has not been built. The question is: what do you use to build it?
How DBT Training Gives You a Clear Clinical Roadmap
Dialectical Behavior Therapy was originally designed for clients with chronic suicidality and severe emotion dysregulation, exactly the population that makes standard EMDR protocols challenging. Linehan's foundational research demonstrated that a structured, skills-based approach to emotion regulation could reduce self-harm, hospitalizations, and treatment dropout in clients who had been considered "too difficult" for traditional therapy. Sound familiar?
For EMDR and trauma therapists, DBT training offers something specific and practical: a map for the terrain your clients are navigating between sessions. Instead of improvising crisis response, you have a shared toolkit. Instead of hoping your clients can manage activation until you see them next, you have taught them specific skills to do exactly that.
Why is DBT training especially important for EMDR therapists with high-risk caseloads? Because the research on integrating DBT with exposure-based therapies shows that DBT skills reduce the between-session crises that derail trauma processing. When your clients have distress tolerance and emotion regulation skills in their toolkit, EMDR prep phases become more stable, reprocessing holds longer, and you spend less of your clinical time doing crisis management instead of trauma work.
And importantly: you do not need to run a full DBT program to benefit from this. An introductory DBT training gives you enough of the skills framework to integrate it meaningfully into your existing EMDR practice. Think of it as adding a precision instrument to your toolkit, not rebuilding your whole approach from scratch.
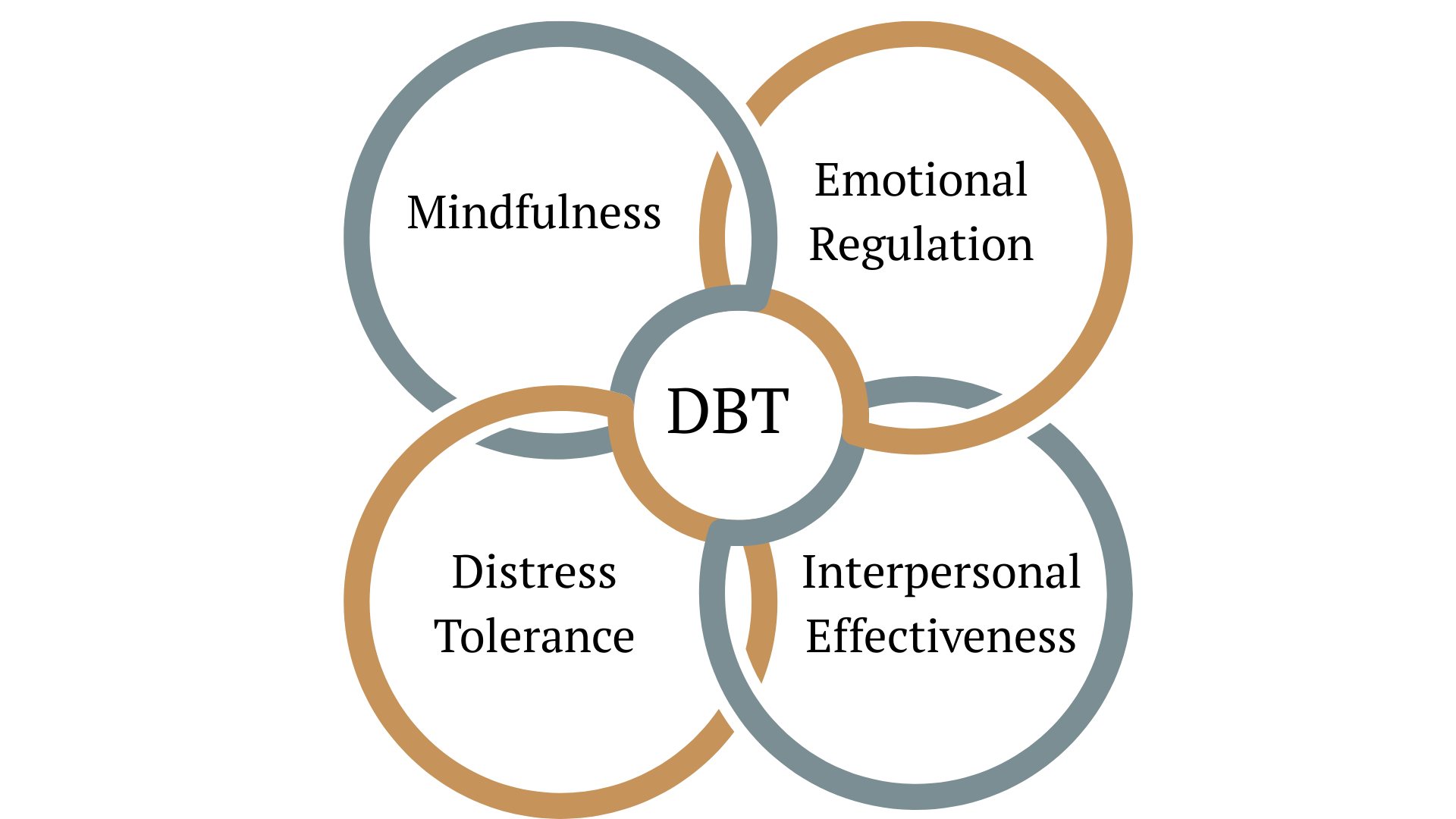
Four Ways DBT Skills Strengthen EMDR Preparation and Phase Work
1. Stabilization Skills Before EMDR: Building Tolerance for Affect
DBT's distress tolerance and emotion regulation skills are natural complements to EMDR Phase 2 preparation work. Teaching clients TIPP, ACCEPTS, or PLEASE before you begin reprocessing means they arrive at reprocessing sessions with more capacity, not less. The window of tolerance expands because you have been systematically building it, not just hoping it will be wide enough when you need it.
2. Risk Reduction: DBT Tools for Suicidality and Self-Harm
One of the most concrete applications of DBT skills for high-risk clients is safety planning that actually works. Studies on DBT for suicidal and self-harming clients show that specific skill sets, particularly crisis survival skills and chain analysis, reduce self-harm and suicidal behavior even in clients with high-acuity presentations. Integrating these into your EMDR work means you have a structured response to between-session crises, not just a safety contract and a prayer.
3. Nervous-System Regulation: Pairing DBT with a Polyvagal Lens
DBT's physiological regulation skills, particularly paced breathing and temperature-based interventions, map cleanly onto a polyvagal framework. When you understand the nervous system underpinnings of trauma responses, you can titrate skill use more precisely. You are not just teaching coping strategies. You are helping clients develop autonomic flexibility, which is exactly what sustained EMDR reprocessing requires.
4. Ethical Scaffolding: DBT and Your Scope-of-Practice Decisions
Perhaps the least-discussed benefit of DBT training for trauma therapists is the ethical clarity it provides. When you have a documented, evidence-based framework for managing self-harm and suicidality, your scope-of-practice decisions become more defensible and more confident. You are not winging it. You are applying evidence-based DBT approaches in a systematic way, which matters enormously both for client safety and for your own protection as a clinician.
From Burnout to Containment: What Changes When You Have Skills to Lean On
There is a particular kind of exhaustion that comes from working without a net. When a client is in crisis and your response is improvised, even if it is a good improvisation, your nervous system registers the uncertainty. Over time, that uncertainty accumulates. Research on compassion fatigue consistently identifies a lack of clinical structure as one of the strongest predictors of therapist burnout in high-acuity settings.
When you add a DBT framework to your practice, something subtle shifts. The conversation with your high-risk client stops being "let's get through this crisis together" and starts being "let's use the tools we've been building." That shift, from clinician-as-sole-lifeline to clinician-and-client-with-a-shared-plan, is not just better for clients. It is protective for you.
You stop being the only thing standing between your client and chaos. The skills are there. The framework is there. You built it together. And that changes the felt sense of your work in ways that are hard to fully describe until you've experienced it.
What to Look For in DBT Training as a Trauma and EMDR Therapist
Not all DBT training is created equal, and if you are an EMDR clinician looking to deepen your high-acuity work, the standard DBT certification track may not be the right starting point. Here is what actually matters:
- Trauma-informed application. Standard DBT was not designed with trauma at the center. Look for training that adapts the skills framework through a trauma lens, so the skills you teach are both effective and safe for clients who are processing past injury.
- Nervous-system awareness. DBT skills work better when they are understood through a polyvagal or somatic lens. Training that integrates this perspective will help you teach the skills more precisely and with more clinical confidence.
- Flexible application over rigid protocol. You are not trying to become a DBT therapist. You are adding DBT skills to an existing EMDR practice. Look for training that explicitly supports flexible, integrated use, not full-model compliance.
- Trainer with real high-acuity experience. There is a meaningful difference between someone who has studied DBT and someone who has spent years applying it with the kinds of clients you see every day. That lived clinical experience shapes how the skills are taught, contextualized, and adapted.
Do I need to run a full gold-standard DBT program to benefit from DBT training in my EMDR practice? No. Integrating DBT skills into complex trauma EMDR work does not require you to operate a full DBT program. What you need is a working knowledge of the core skill modules, how to teach them, when to lean on them, and how to connect them to the EMDR work you are already doing. That is exactly what a focused introductory training provides.
How Do DBT Skills Practically Show Up in EMDR Work With High-Risk Clients?
In practice, it looks like this. You are doing EMDR Phase 2 preparation with a client who has a history of self-harm when overwhelmed. Instead of relying solely on safe-place imagery and container exercises, you spend three sessions teaching TIPP and ACCEPTS as concrete between-session tools. You build a crisis plan together using a DBT chain analysis structure. By the time you begin memory assessment, your client has a toolkit. They know what to do when activation peaks at 2 a.m. and you are not available.
It looks like a client who has been stuck in EMDR prep for months because they keep destabilizing between sessions, who starts showing up to sessions regulated enough to actually begin reprocessing, after you shifted the focus to Phase 1 stabilization per ISTSS guidelines using DBT emotion regulation skills.
It looks like you, finishing a session with a high-acuity client and feeling clear rather than depleted. Because the session had structure. And structure, as DBT training programs consistently emphasize, is what makes sustainable trauma work possible.
Next Step: Learn Foundational DBT Skills Live
If any of this resonates with you, the most direct next step is Intro to DBT: Skills Training for the Attuned Trauma Therapist, a focused, live online training designed specifically for trauma and EMDR therapists who are working with high-acuity clients and want a practical, immediately usable DBT skills framework. Three hours. Skills focus. High-risk lens. No prerequisite certification required.
This is not theory overload. It is the right-sized starting point for adding DBT to the work you are already doing. You will leave with concrete skills to teach, a clearer framework for managing between-session crises, and the kind of clinical confidence that comes from knowing you are not improvising. DBT for trauma and complex trauma is a distinct clinical skill set, and this training will give you a strong, grounded foundation in it.
Your clients deserve a therapist who has the tools to go the distance with them. So do you.
References
Linehan, M. M., Armstrong, H. E., Suarez, A., Allmon, D., & Heard, H. L. (1991). Cognitive-behavioral treatment of chronically parasuicidal borderline patients. Archives of General Psychiatry, 48(12), 1060-1064. https://doi.org/10.1001/archpsyc.1991.01810360024003
Bisson, J. I., Roberts, N. P., Andrew, M., Cooper, R., & Lewis, C. (2013). Psychological therapies for chronic post-traumatic stress disorder (PTSD) in adults. Cochrane Database of Systematic Reviews, 12. https://doi.org/10.1002/14651858.CD003388.pub4
Cloitre, M., Courtois, C. A., Ford, J. D., Green, B. L., & Alexander, P. (2012). The ISTSS expert consensus treatment guidelines for complex PTSD in adults. International Society for Traumatic Stress Studies. https://www.scribd.com/document/327508064/ISTSS-Complex-Trauma-Treatment-Guidelines-2012-Cloitre-Courtois-Ford-Green-Alexander-B
DBT Training Australia. (n.d.). DBT skills training. https://dbttrainingaustralia.au/training/40
EMDRIA. (n.d.-a). Adapting the 8 phases: Considerations for working with clients at an elevated risk for suicide. https://www.emdria.org/blog/adapting-the-8-phases-considerations-for-working-with-clients-at-an-elevated-risk-for-suicide/
EMDRIA. (n.d.-b). Phase 2 practice tips for EMDR therapists. https://www.emdria.org/blog/phase-2-practice-tips-for-emdr-therapists/
eCare Behavioral Institute. (n.d.). Using dialectical behavior therapy (DBT) for trauma and complex trauma. https://www.ecarebehavioralinstitute.com/courses/using-dialectical-behavior-therapy-dbt-for-trauma-complex-trauma/
Fonzo, G. A., & Etkin, A. (2017). Affective neuroimaging in generalized anxiety disorder: An integrated review. Dialogues in Clinical Neuroscience, 19(2), 107-121. https://doi.org/10.31887/DCNS.2017.19.2/gfonzo
Harned, M. S., Korslund, K. E., & Linehan, M. M. (2014). A pilot randomized controlled trial of Dialectical Behavior Therapy with and without the DBT Prolonged Exposure protocol for suicidal and self-injuring women with borderline personality disorder and PTSD. Behaviour Research and Therapy, 55, 7-17. https://doi.org/10.1016/j.brat.2014.02.002
International Society for Traumatic Stress Studies. (n.d.). Phase one: Safety and stabilization. https://iptrauma.org/docs/the-triphasic-model-for-treating-trauma/phase-one-safety-and-stabilization/
Kliem, S., Kroger, C., & Kosfelder, J. (2010). Dialectical behavior therapy for borderline personality disorder: A meta-analysis using mixed-effects modeling. Journal of Consulting and Clinical Psychology, 78(6), 936-951. https://doi.org/10.1037/a0021015
Linardon, J., Fairburn, C. G., Fitzsimmons-Craft, E. E., Wilfley, D. E., & Brennan, L. (2017). The empirical status of the third-wave behaviour therapies for the treatment of eating disorders. Clinical Psychology Review, 58, 125-140. https://doi.org/10.1016/j.cpr.2017.10.005
McHugh, R. K., Whitton, S. W., Peckham, A. D., Welge, J. A., & Otto, M. W. (2013). Patient preference for psychological vs. pharmacological treatment of psychiatric disorders. Journal of Clinical Psychiatry, 74(6), 595-602. https://doi.org/10.4088/JCP.12r07757
Shapiro, F., & Maxfield, L. (2002). Eye movement desensitization and reprocessing (EMDR): Information processing in the treatment of trauma. Journal of Clinical Psychology, 58(8), 933-946. https://doi.org/10.1002/jclp.10068
Stamm, B. H. (2010). The concise ProQOL manual (2nd ed.). ProQOL.org. https://doi.org/10.1037/t07192-000
Trauma Therapist Institute. (n.d.). Complex trauma and EMDR: A comprehensive training guide for clinicians. Brain-Based EMDR. https://www.brainbasedemdr.com/blog/complex-trauma-emdr-a-comprehensive-training-guide-for-clinicians
Cannon Psychology. (n.d.). EMDR Phase 2: Preparation. https://cannonpsychology.com/blog-emdr-therapy-california-nevada-idaho/emdr-phase-two-preparation
Stay connected with fun info, news, promotions and updates!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.