
EFT Tapping for Trauma: What the Research Actually Says (And How to Use It Clinically)
Apr 13, 2026
Read Time: 10 Minutes
Written by: The TTI Team
You’ve probably heard the word “tapping” come up in training, a conversation with a colleague, or from a client who tried it between sessions. Maybe you looked it up and got a mix of wellness blogs, YouTube tutorials, and one overly enthusiastic energy healer. Understandable if you moved on.
But here’s the thing. EFT tapping, meaning Emotional Freedom Techniques, is not a wellness trend. It is a clinically researched, evidence-based intervention with over 200 peer-reviewed trials behind it, five meta-analyses, and an APA evidence-based designation. And for therapists working with trauma clients, particularly the ones who flood, freeze, or simply cannot get traction through talk or even standard trauma protocols, it offers something genuinely worth knowing about.
This post is about what the research actually shows, how EFT tapping works neurologically, and how it fits into trauma treatment in a practical, phase-oriented way. No energy field theory. No promises of miracle cures. Just an honest clinical picture.
What EFT Tapping Actually Is (And What It Is Not)
First, a quick clarification worth making. “EFT” is unfortunately used as an acronym for three different things in mental health: Emotional Freedom Techniques (tapping), Emotionally Focused Therapy (Sue Johnson’s couples model), and Emotion-Focused Therapy (Les Greenberg’s individual approach). This post is about the first one only. If you’ve ever Googled EFT and ended up reading about attachment bonds and pursue-withdraw cycles, that’s why.
Emotional Freedom Techniques is a body-based psychological intervention that combines three elements in a single protocol:
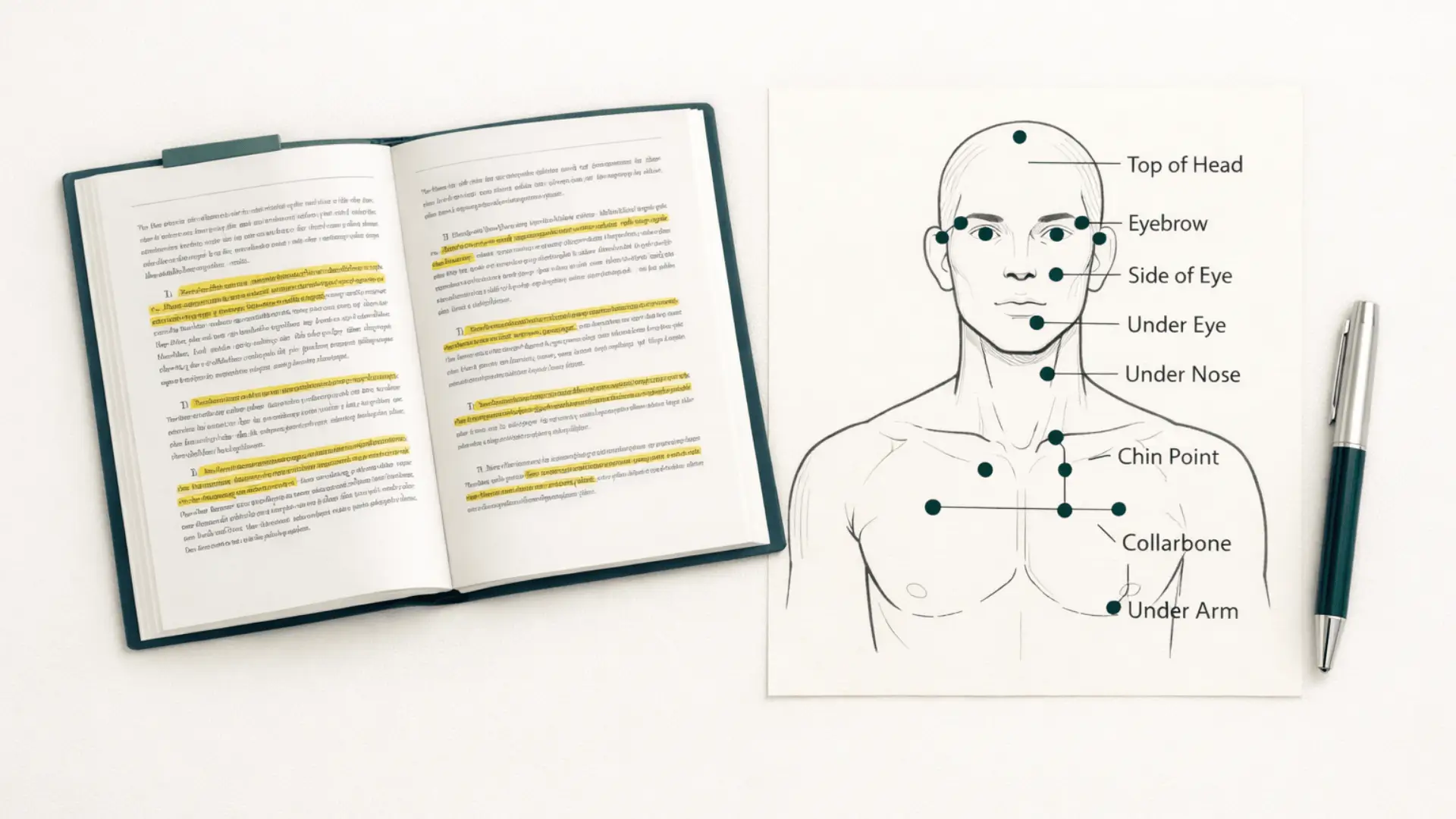
- Somatic stimulation: tapping with the fingertips on nine specific acupressure points on the face, chest, and hands
- Focused attention: maintaining conscious attention on a specific distressing issue, memory, or body sensation
- Cognitive reframing: a set-up statement that pairs acknowledgment of the problem with a self-acceptance phrase
The set-up statement is the part that tends to surprise people. It follows this structure: “Even though [specific problem or feeling], I deeply and completely accept myself.” Before tapping begins, the client rates their distress on a Subjective Units of Distress (SUD) scale from 0 to 10. After each round of tapping through the points, the SUD is re-rated. The process continues until distress decreases to a manageable or neutral level.
What this means clinically is that EFT is not a relaxation technique and it is not talk therapy. It is an exposure-based intervention with a somatic component layered on top. The client is not avoiding the distressing material. They are actively holding it in mind while simultaneously engaging the body in a way that appears to interrupt the stress response. That combination is what makes it interesting from a trauma treatment perspective.
Why Clinicians Are Skeptical (And Why That Skepticism Is Worth Revisiting)
The skepticism is fair. EFT has roots in Thought Field Therapy, developed by Roger Callahan in the 1980s, which was itself rooted in the idea of energy meridians borrowed from traditional Chinese medicine. Gary Craig simplified Callahan’s protocol in the 1990s and introduced it to a wide audience, initially framing it heavily in the language of “energy fields” and “disruptions in the body’s energy system.” That language made many evidence-based clinicians understandably cautious. It still does.
But here is where the story shifts. Current research on EFT does not lean on subtle energy theory. It focuses on measurable neurobiological and physiological mechanisms, which we will get to in a moment. And the clinical trial base has grown substantially.
So, is EFT tapping evidence-based for trauma? The short answer is yes, more than most clinicians realize. A 2022 systematic review published in Frontiers in Psychology identified 56 randomized controlled trials of Clinical EFT and found it met APA criteria as an evidence-based practice for anxiety, depression, phobias, and PTSD. The US Veterans Administration has designated it “generally safe.” The APA has offered continuing education credits for EFT courses since 2011.
The effect sizes are not modest. Meta-analyses show a large treatment effect for PTSD (d = 2.96), anxiety (d = 1.23), and depression (d = 1.31). To put that in context, these are effect sizes that exceed those reported for many pharmacological interventions and for conventional psychotherapy in comparable populations. Ninety-six percent of published studies show results in EFT’s favor. The dropout rate in PTSD trials is also notably low, which matters clinically because it suggests clients are not finding the process intolerable.
A 2023 updated systematic review and meta-analysis published in Frontiers in Psychology drew on trials covering veterans, sexual violence survivors, disaster survivors, prison populations, and adolescents. Consistent positive outcomes across that range of populations and settings is a meaningful signal.
How Does EFT Tapping Work for PTSD? The Neurobiological Case
If the research has convinced you to keep reading, the next question is the mechanism. How does tapping on your collarbone and the side of your eye change anything about trauma?
A 2025 review by David Feinstein published in Frontiers in Psychology synthesizes over two decades of research into what is actually happening physiologically during an EFT session. The findings are not speculative. Tapping appears to generate electrochemical signals that downregulate limbic activation, including in the amygdala, which is the brain’s threat detection system. fMRI research has shown reduced arousal in brain regions associated with fear and stress responses following acupoint stimulation. Harvard Medical School’s ten-year investigation into acupressure and the amygdala found that stimulation of these points produced rapid downregulation of limbic arousal, sometimes within seconds.
On the hormonal side, a randomized controlled trial by Church et al. found that a single hour of EFT produced an average cortisol reduction of 24%, compared to no significant change in the talk therapy group and the no-treatment control group. You can read the full systematic review here. Lower cortisol means a less activated stress response. For clients who are chronically dysregulated, that is not a small thing.
Perhaps the most clinically significant piece is how EFT appears to facilitate memory reconsolidation. When a distressing memory is reactivated while the client is simultaneously in a state of physiological calm created by the tapping, the brain registers a mismatch between what it expected (distress) and what it is experiencing (relative calm). That prediction error is exactly the condition memory reconsolidation theory says is needed to update the emotional charge of a memory. The tapping does not suppress the memory. It creates the conditions for the memory’s emotional associations to be neurologically rewritten.
This is the same mechanism EMDR researchers point to. Which brings us to the clinical application.
EFT Tapping Phase-Oriented Trauma Treatment: The Two Clinical Modes
One of the reasons EFT can feel unclear to trauma therapists is that it gets presented as a single technique when it actually operates in two meaningfully different modes. Understanding this distinction is what makes it clinically useful rather than just interesting.
Phase 1: Nervous System Regulation
In the first mode, EFT is used as a regulation and stabilization tool. The target is not a traumatic memory. The target is a current state: anxiety, activation, a feeling in the body, a chronic pattern of overwhelm. The goal is to reduce arousal, expand the window of tolerance, and build nervous system capacity before any trauma processing begins.
This is particularly relevant for clients who arrive in a dysregulated state, who flood easily, or who have been unable to access trauma processing because their baseline activation is simply too high. Used in Phase 1, EFT functions similarly to other somatic regulation approaches, but with the addition of the cognitive and exposure elements baked in from the start.
You can read more about how EFT supports regulation as a foundation for deeper trauma work in this clinical conversation with Dr. Robert Schwarz on the TTI site.
Phase 2: Titrated Trauma Processing
In the second mode, EFT moves into the work of approaching traumatic material. This is where the specific trauma-focused techniques come in. The key point is that EFT does not require full re-narration of the traumatic event. The client does not have to tell the whole story to get therapeutic movement. That makes it particularly useful for clients who are high-risk for flooding during more direct exposure approaches.
Key EFT Techniques for Trauma Therapists
If you are thinking about how EFT tapping clinical applications might look in practice, these are the three techniques most relevant to trauma work.
The Tearless Trauma Technique
This approach is designed for memories that carry a very high emotional charge, where direct engagement would risk flooding or overwhelm. The client thinks about the event without narrating it, estimates their SUD rating, and taps on that anticipated distress rather than the memory itself. Over successive rounds, the emotional charge reduces enough for more direct work to become possible. It is a way of approaching the edge without stepping over it.
The Tell the Story Technique
Once regulation is more established, the client narrates the traumatic event as if telling a story, pausing and tapping whenever emotional intensity rises above a manageable threshold. The therapist watches for spikes in distress and prompts tapping at those points. Processing happens in titrated steps rather than through full immersion. This is how EFT stays within the window of tolerance even when working with specific traumatic memories.
The Personal Peace Procedure
This is a treatment planning tool. The client generates a list of specific troubling memories, events, or issues and works through them systematically using EFT, starting with lower-charge items and building up. For clients with complex or layered trauma histories, this provides a structured map for the work rather than a random approach to whatever is most activated on a given day.
For a broader look at how somatic approaches integrate with trauma processing, this piece on somatic EMDR training covers the clinical thinking around titration, pendulation, and body-based work that also applies to EFT.
EFT Tapping vs. EMDR for Trauma: How They Fit Together
How is EFT tapping different from EMDR? This comes up a lot. Both are exposure-based. Both facilitate memory reconsolidation. Neither requires full re-narration. The main differences are in mechanism and structure. EMDR uses bilateral stimulation across a formal eight-phase protocol. EFT uses acupoint tapping across the two clinical modes described above. A 2011 controlled trial, the first ever direct comparison of EMDR and EFT for PTSD, found similar effect sizes across both treatment groups in an equal number of sessions.
What this means practically is that EFT is not a replacement for EMDR. For clinicians already trained in EMDR, EFT offers an additional tool, particularly useful in Phase 1 regulation, for clients who are not yet ready for full trauma reprocessing, or as a between-session self-help skill that clients can apply independently.
The connection to other modalities is also worth naming. The self-acceptance language in the EFT set-up statement draws on ACT-informed principles of psychological flexibility. The somatic regulation mechanism connects directly to polyvagal-informed practice: tapping appears to work partly through vagal tone, interrupting the sympathetic stress response and creating the physiological conditions for social engagement and processing. Dr. Robert Schwarz, one of the field’s most experienced EFT trainers, explored this connection in depth in his 2018 chapter, Energy Psychology, Polyvagal Theory, and the Treatment of Trauma, published in Porges and Dana’s Clinical Applications of the Polyvagal Theory (W. W. Norton & Company).
Who EFT Works Well With

The research base covers a wide range of presentations and populations. The strongest evidence exists for:
- Veterans with PTSD, including combat trauma and moral injury
- Survivors of sexual violence
- Disaster and genocide survivors
- Clients with anxiety disorders, including phobias and generalized anxiety
- Clients with depression, including moderate-severity presentations
- Clients with chronic pain where psychological distress is a significant component
A 2024 meta-analysis of 18 randomized controlled trials, published in the Journal of Clinical Medicine, found an overall effect size of 1.268 for EFT in reducing depressive symptoms, with group-based delivery showing particularly strong results and shorter interventions performing well in moderate-severity presentations.
For complex trauma presentations, including clients with dissociative features or layered developmental trauma, EFT can be integrated carefully, particularly in Phase 1 where regulation is the focus. The PTSD clinical guidelines for EFT include a stepped-care approach for more complex cases.
One safety point worth noting explicitly: across 2,000+ research participants in clinical trials, no adverse events have been reported. The neural changes research, including a fMRI study of chronic pain sufferers published in Complementary Therapies in Clinical Practice, showed significant reductions in pain severity, anxiety, and depression alongside measurable changes in brain connectivity patterns after a six-week EFT intervention.
Do You Need Special Certification to Use EFT Tapping with Clients?
This is one of the most common questions clinicians have, and the honest answer is: most licensed therapists can incorporate EFT into their practice after appropriate clinical training, without needing a separate licensure pathway.
The important distinction is between self-help or wellness EFT and Clinical EFT, which is the manualized, research-validated form used in the trials cited throughout this post. Clinical EFT requires understanding the full protocol, the phase-oriented framework, and the specific techniques relevant to trauma populations. The tearless trauma technique, the tell the story technique, and the personal peace procedure each require clinical skill and judgment to apply well. You are not just tapping along with a client. You are making decisions about pacing, titration, and when to move between modes.
For licensed clinicians, the priority is competence, not a credential. Learning EFT from someone with genuine clinical depth, a strong grounding in trauma treatment, and real familiarity with the research base is what matters most.
Ready to Learn EFT Tapping in a Trauma Treatment Context?
If you’ve read this far and found yourself thinking “I want to actually learn how to do this,”we have something for you.
EFT Tapping Training for Trauma Therapists is a live, full-day training with Dr. Robert Schwarz, PsyD, DCEP, one of the most experienced EFT trainers in the field and a licensed psychologist with 40 years of trauma treatment experience. Bob served as Executive Director of the Association for Comprehensive Energy Psychology for 16 years and has trained clinicians in EFT across international settings.
- Thursday, July 16, 2026 | 10:00 am – 5:30 pm Central | Live online
- 6 CEs | ASWB, NBCC
- Open to all licensed clinicians. No prior EFT experience required.
You will leave with the complete EFT protocol, the tearless trauma and tell the story techniques, the personal peace procedure for treatment planning, and a clear understanding of how and why EFT belongs in phase-oriented trauma work.
References
Church, D., Stapleton, P., Vasudevan, A., & O’Keefe, T. (2022). Clinical EFT as an evidence-based practice for the treatment of psychological and physiological conditions: A systematic review. Frontiers in Psychology, 13, Article 951451. https://doi.org/10.3389/fpsyg.2022.951451
Church, D., & Feinstein, D. (2017). Guidelines for the treatment of PTSD using Clinical EFT (Emotional Freedom Techniques). Healthcare, 5(4), Article 49. https://doi.org/10.3390/healthcare5040049
Clond, M., & Sebastian, B. (2023). Emotional freedom techniques for treating post-traumatic stress disorder: An updated systematic review and meta-analysis. Frontiers in Psychology, 14, Article 1195286. https://doi.org/10.3389/fpsyg.2023.1195286
Feinstein, D. (2025). How tapping works: Physiological and psychological mechanisms in energy psychology treatments. Frontiers in Psychology, 16, Article 1660375. https://doi.org/10.3389/fpsyg.2025.1660375
Karatzias, T., Power, K., Brown, K., McGoldrick, T., Begum, M., Young, J., Loughran, P., Chouliara, Z., & Adams, S. (2011). A controlled comparison of the effectiveness and efficiency of two psychological therapies for posttraumatic stress disorder: Eye movement desensitization and reprocessing vs. emotional freedom techniques. Journal of Nervous and Mental Disease, 199(6), 372–378. https://doi.org/10.1097/NMD.0b013e31821cd262
Lin, Y., Fang, S., Li, Y., & Zhang, Y. (2024). The effectiveness of emotional freedom techniques for depressive symptoms: A meta-analysis. Journal of Clinical Medicine, 13(21), Article 6481. https://doi.org/10.3390/jcm13216481
Schwarz, R. (2018). Energy psychology, Polyvagal Theory, and the treatment of trauma. In S. W. Porges & D. Dana (Eds.), Clinical applications of the polyvagal theory: The emergence of polyvagal-informed therapies (pp. 270–284). W. W. Norton & Company.
Stapleton, P., Baumann, O., O’Keefe, T., & Bhopti, S. (2022). Neural changes after Emotional Freedom Techniques treatment for chronic pain sufferers. Complementary Therapies in Clinical Practice, 49, Article 101653. https://doi.org/10.1016/j.ctcp.2022.101653
Stay connected with fun info, news, promotions and updates!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.



