
DBT and EMDR for Complex Trauma: Why Stabilization Before Insight Protects Clients (and Clinicians)
Apr 06, 2026

When EMDR Isn't Enough on Its Own
Picture this: You're twelve minutes into an EMDR reprocessing session when your client's eyes go flat. They're gone. Not in the therapeutic sense of deep processing, but actually gone. Dissociated. The trauma material surfaced faster than their window of tolerance could hold it, and now you're doing crisis management instead of trauma therapy.
Sound familiar? If you work with complex trauma, it probably does.
EMDR is one of the most evidence-backed trauma therapies we have. Research consistently shows it reduces PTSD symptoms faster than many traditional talk therapies. But for clients carrying complex PTSD, borderline personality disorder traits, chronic suicidality, or long histories of self-harm, standard EMDR prep phases can feel like trying to build a house on sand. The foundation isn't there yet.
That's where DBT comes in. Not as a competing modality, not as a detour, but as the stabilization scaffold that makes meaningful EMDR work possible. The phrase "stabilization before insight" isn't a delay tactic or a way to avoid doing the hard work. It's an ethical stance. It's you, as a clinician, recognizing that phase-oriented trauma treatment exists for a reason.
In this post, we're going to break down how DBT skills for EMDR preparation actually work in practice, which specific skill sets matter most, and how this integrated approach protects not just your clients but you as the clinician holding the space.
Why High-Risk, Complex Trauma Clients Need More Than Insight
Here's the honest truth about complex trauma: insight alone doesn't heal it. Your client can intellectually understand that their hypervigilance came from growing up in a chaotic household and still completely fall apart when their partner raises their voice. That's because complex trauma and attachment injury don't live in the thinking brain. Research on Marsha Linehan's biosocial theory tells us that chronic emotion dysregulation, the kind that shows up in many complex trauma presentations, is the result of a biologically sensitive nervous system meeting an emotionally invalidating environment. Over and over again.
The clients we're talking about here often present with a constellation of challenges: chronic suicidal ideation, self-harm behaviors, dissociation, and volatile relationships. These aren't just "difficult cases." They're people whose nervous systems learned to operate in survival mode as a primary strategy. Studies on EMDR for complex PTSD consistently note that standard protocols need adaptation for this population precisely because of the emotion dysregulation piece.
And clinicians feel it too. Working with high-risk trauma clients without a clear framework can leave you feeling like you're improvising a high-wire act without a net. The fear of doing harm, the ongoing crisis management, the quiet anxiety about scope-of-practice boundaries, it adds up. It's a fast track to burnout.
How DBT Provides Structure for High-Risk EMDR Cases
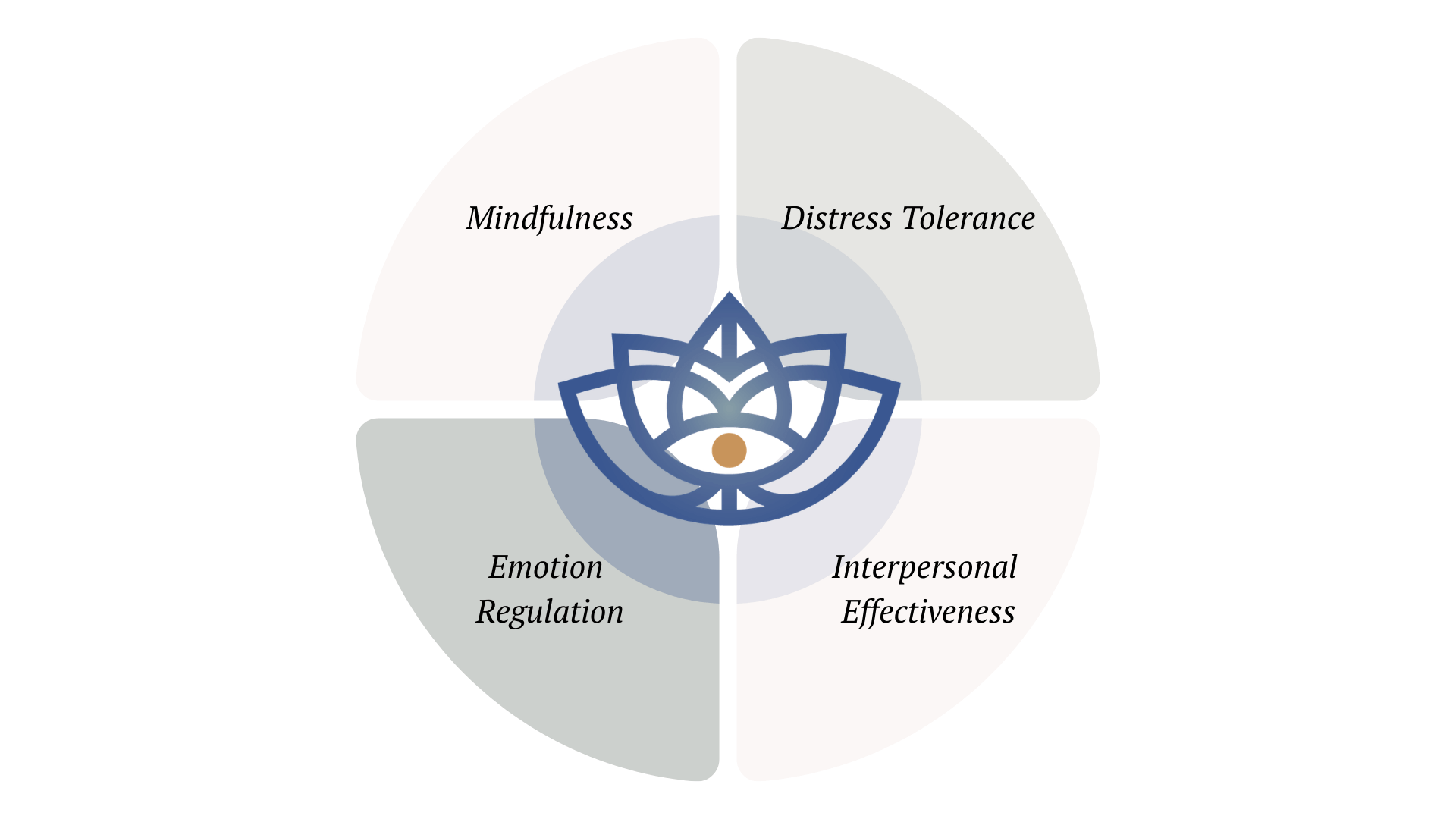
Think of DBT's four skill modules not as a separate treatment track but as a clinical containment scaffold. DBT-informed approaches give you, and your client, a shared language and a structured toolkit before you wade into trauma processing. Here's how each module supports the work:
- Mindfulness: Grounds clients in present-moment awareness, a prerequisite for the dual attention required in EMDR reprocessing.
- Distress Tolerance: Equips clients with crisis survival tools so that between-session activation doesn't automatically lead to the ER.
- Emotion Regulation: Builds the nervous system capacity needed to tolerate memory processing without flooding.
- Interpersonal Effectiveness: Stabilizes the therapeutic relationship and the client's external support system, which matters enormously when trauma work gets hard.
Importantly, this doesn't mean you need to become a DBT therapist or run a full DBT program. Foundational DBT skills can be woven into existing EMDR prep work without overhauling your whole practice. The goal is structure, not a new specialty certification.
Do I need full-model DBT training before I can use DBT skills alongside EMDR? The short answer is no. What you need is a solid working knowledge of the core skill sets, how to teach them, how to reinforce them, and how to help clients apply them in moments of activation. Integrating DBT into exposure-based trauma work is a clinical skill in itself, one that's very much learnable without a full DBT certification.
Three DBT Skill Sets That Directly Support EMDR Preparation
1. Mindfulness for Orientation and Dual Awareness
EMDR requires something called dual awareness: the ability to stay grounded in the present while accessing past memory material. Without it, clients don't process. They either go blank (freeze/dissociate) or they get flooded. Mindfulness practices build this capacity directly. Short, non-flooding exercises that help clients track the difference between "then" and "now" are essential groundwork. Think of it as calibrating the instrument before the surgery. EMDR Phase 2 stabilization works best when mindfulness is already part of the client's repertoire.
2. Distress Tolerance for Managing Activation Between Sessions
One of the hardest realities of doing EMDR with complex trauma clients is that trauma material doesn't stay neatly inside the therapy hour. Clients go home. Big material surfaces in the middle of the night, or on the drive to pick up their kids, or in the grocery store. Without distress tolerance skills, that activation can spiral into crisis: self-harm, hospitalizations, phone calls that pull you both back to ground zero. Research on emotion dysregulation in PTSD makes clear that between-session coping capacity is one of the key variables in trauma treatment outcomes.
Teaching TIPP skills (Temperature, Intense exercise, Paced breathing, Progressive relaxation), ACCEPTS distraction strategies, and self-soothe practices gives clients a bridge to safety between sessions. This isn't avoidance. It's survival until the next session.
3. Emotion Regulation for Vulnerability Factors
EMDR reprocessing goes better when clients aren't already running on empty. DBT's emotion regulation module addresses exactly this, specifically the vulnerability factors that make the nervous system less able to tolerate activation: poor sleep, skipped meals, substance use, chronic illness. Skills like PLEASE (treat PhysicaL illness, balanced Eating, Avoid mood-altering drugs, balanced Sleep, Exercise), Build Positive Experiences, and Mastery aren't soft add-ons. They're readiness builders. A client who has slept, eaten, and built even one small positive experience this week is a very different nervous system to work with than one who hasn't. The evidence on phase-oriented trauma treatment supports this kind of systematic stabilization before diving into reprocessing.
Case Vignette: When EMDR Pauses and DBT Steps In

Consider a composite client we'll call Maya. Maya is 34, a survivor of childhood emotional abuse and neglect, and she came to therapy specifically requesting EMDR. She'd read about it. She was ready. Or so she thought.
In the first few sessions, Maya's assessment revealed a long history of passive suicidal ideation, occasional cutting when overwhelmed, and significant dissociative tendencies during stress. According to EMDRIA's guidance on adapting the 8 phases for suicidal clients, diving into reprocessing with Maya's current stabilization level would be clinically contraindicated.
So EMDR paused. Not abandoned. Paused.
For six weeks, the work shifted to DBT-informed stabilization. Maya learned mindfulness through brief, body-based exercises that helped her stay present without flooding. She practiced distress tolerance skills for the moments when old memories intruded unbidden. She started tracking her sleep, eating more regularly, and using a simple mood log to notice patterns. The therapeutic relationship deepened because she felt met, not pushed. This reflects what ISTSS complex trauma treatment guidelines describe as Phase 1 stabilization work.
When EMDR resumed, it was different. Maya could hold dual awareness. When a memory surfaced with intensity, she had tools to work with the activation rather than being swallowed by it. Six weeks of DBT-informed preparation didn't slow her healing. It made it possible.
When should you pause EMDR and shift more heavily into DBT-informed stabilization? Watch for repeated session derailments, ongoing suicidality or active self-harm, significant dissociation during memory assessment, and a lack of basic external supports. These are signals, not failures. They're the client's nervous system telling you the scaffold isn't ready yet. Stabilization before EMDR is not just best practice. It's how you honor the client's actual window of tolerance.
Protecting Clinicians: DBT Skills as Burnout and Risk-Reduction Tools
Here's something that doesn't get said enough: having a DBT framework protects you as the clinician, not just your clients. When you're working with high-acuity trauma clients without a clear structure, you end up improvising in crisis. A lot. That improvisation, however skilled, carries a quiet weight. The question "Am I doing the right thing?" can follow you home. Research on therapist burnout consistently identifies a lack of clinical structure as one of the key contributors to compassion fatigue.
DBT gives you something to stand on. A shared treatment framework, clear skill sets to teach, observable indicators of progress. That structure is also what allows you to answer scope-of-practice questions with confidence. You're not "winging it" with a suicidal client. You're applying evidence-based DBT skills for high-risk trauma clients in a purposeful, documented way. That matters for consultation, for supervision, and for your own peace of mind.
There's a version of trauma therapist training DBT that frames all of this as clinical responsibility. You became a trauma therapist because you care about helping people heal from the worst things that happened to them. Having the right tools isn't a luxury. It's how you sustain that commitment over a whole career.
Bringing This Into Your Practice: Your First Small Step
You don't need to overhaul your practice to start integrating DBT skills into EMDR prep. Start with two things. First, teach one distress tolerance skill, specifically Paced Breathing or the TIPP technique, as part of your standard EMDR Phase 2 preparation for every complex trauma client. Frame it as a between-session support tool, not an add-on. Second, add a brief mindfulness orientation exercise at the start of each EMDR session to anchor dual awareness before you begin. Practical DBT skills for EMDR clinicians can be integrated incrementally without disrupting your existing work.
How does DBT actually support EMDR work with complex trauma clients? The short answer is that it addresses what EMDR alone can't: the regulation deficits, crisis survival skills, and vulnerability factors that make reprocessing both possible and safe. DBT doesn't compete with EMDR. It creates the conditions EMDR needs to work. As Francine Shapiro's original work emphasized, client preparation and stabilization are not preliminary steps. They are the work.
Ready to go deeper?
If you want a live, practical walk-through of DBT skills for high-acuity trauma work, including exactly how they complement EMDR and when to use which skills in which phase, join us for Intro to DBT: Skills Training for the Attuned Trauma Therapist. This course is built for EMDR clinicians who want clinical structure, not theory overload. Real skills, immediately applicable, designed for the complexity of the clients you're actually seeing.
Your clients are ready when their nervous systems are ready. Let's build that readiness together.
References
Bisson, J. I., Roberts, N. P., Andrew, M., Cooper, R., & Lewis, C. (2013). Psychological therapies for chronic post-traumatic stress disorder (PTSD) in adults. Cochrane Database of Systematic Reviews, 12. https://doi.org/10.1002/14651858.CD003388.pub4
Brown, L. A., Zandberg, L. J., & Foa, E. B. (2019). Mechanisms of change in prolonged exposure therapy for PTSD: Implications for clinical practice. Journal of Psychotherapy Integration, 29. https://doi.org/10.1037/int0000109
Harned, M. S., Korslund, K. E., & Linehan, M. M. (2014). A pilot randomized controlled trial of Dialectical Behavior Therapy with and without the DBT Prolonged Exposure protocol for suicidal and self-injuring women with borderline personality disorder and PTSD. Behaviour Research and Therapy, 55. https://doi.org/10.1016/j.brat.2014.02.002
Linehan, M. M., Armstrong, H. E., Suarez, A., Allmon, D., & Heard, H. L. (1991). Cognitive-behavioral treatment of chronically parasuicidal borderline patients. Archives of General Psychiatry, 48. https://doi.org/10.1001/archpsyc.1991.01810360024003
Mavranezouli, I., Megnin-Viggars, O., Daly, C., Dias, S., Stockton, S., & Bhutani, G. (2023). Psychological treatments for post-traumatic stress disorder in adults: A network meta-analysis. Frontiers in Psychiatry, 14. https://doi.org/10.3389/fpsyt.2023.1238116
Oken, B. S., Kishiyama, S., Zajdel, D., Bourdette, D., Carlsen, J., Haas, M., Hugos, C., Kraemer, D. F., Lawrence, J., & Mass, M. (2004). Randomized controlled trial of yoga and exercise in multiple sclerosis. Neurology, 62. https://doi.org/10.1212/01.WNL.0000115150.90233.D4
Psychwire. (n.d.). Applied DBT skills for trauma. https://psychwire.com/linehan/applied-dbt-skills-for-trauma
Behavioral Psych Studio. (n.d.). Practical DBT skills for EMDR clinicians. https://behavioralpsychstudio.com/10389-2/
Schnyder, U., Ehlers, A., Elbert, T., Foa, E. B., Gersons, B. P. R., Resick, P. A., Shapiro, F., & Cloitre, M. (2025). Trauma-focused psychotherapies: Update and perspectives. Frontiers in Psychiatry, 16. https://doi.org/10.3389/fpsyt.2025.1538267
Stamm, B. H. (2010). The concise ProQOL manual (2nd ed.). ProQOL.org. https://doi.org/10.1037/t07192-000
Cloitre, M., Courtois, C. A., Ford, J. D., Green, B. L., & Alexander, P. (2012). The ISTSS expert consensus treatment guidelines for complex PTSD in adults. https://www.scribd.com/document/327508064/ISTSS-Complex-Trauma-Treatment-Guidelines-2012-Cloitre-Courtois-Ford-Green-Alexander-B
Shapiro, F., & Maxfield, L. (2002). Eye movement desensitization and reprocessing (EMDR): Information processing in the treatment of trauma. Journal of Clinical Psychology, 58. https://doi.org/10.1002/jclp.10068
International Society for Traumatic Stress Studies. (n.d.). Phase one: Safety and stabilization. https://iptrauma.org/docs/the-triphasic-model-for-treating-trauma/phase-one-safety-and-stabilization/
Centre Self. (n.d.). EMDR Phase 2 stabilization for building resilience. https://centreself.com.au/emdr-phase-two-stabilization-for-building-resilience/
EMDRIA. (n.d.). Adapting the 8 phases: Considerations for working with clients at an elevated risk for suicide. https://www.emdria.org/blog/adapting-the-8-phases-considerations-for-working-with-clients-at-an-elevated-risk-for-suicide/
EMDR Master. (n.d.). Stabilization before EMDR. https://www.emdrmaster.com/stabilization-before-emdr/
Shapiro, F. (1989). Eye movement desensitization: A new treatment for post-traumatic stress disorder. https://francineshapirolibrary.omeka.net/items/show/17178
Harned, M. S. (2022). Integrating dialectical behavior therapy into exposure therapy for complex posttraumatic stress. Eating Disorders Review. https://edr.iaedpfoundation.com/integrating-dialectical-behavior-therapy-into-exposure-therapy-for-complex-posttraumatic-stress/
Stay connected with fun info, news, promotions and updates!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.



