Working with Ego States in the 8 Phases of EMDR
Apr 14, 2026
Reading Time: 10 minutes
Written By: The TTI Team
You are mid-set with a client. Processing has been moving. The SUDS dropped from a 7 to a 4, the client is tracking well, and you are starting to feel that quiet clinical satisfaction that comes when EMDR is doing what it is supposed to do.
Then the client’s eyes go flat. Their voice changes. The SUDS either rockets back to a 9 or plummets to zero, and the person sitting across from you suddenly feels like a different person. Because, in a real clinical sense, it is.
A protective part just showed up. And in that moment, you have a decision to make: Do you keep going with bilateral stimulation? Pause and address the part? Go back to resourcing? If you are like most EMDR-trained clinicians, your basic training gave you a thorough grounding in the standard protocol but probably did not spend much time on what to do when ego states enter the room. That leaves a gap, and with complex trauma clients, it is a gap that shows up constantly.
This article walks through all 8 phases of EMDR and identifies where ego states are most likely to emerge, what they look like in session, and what kinds of EMDR ego state interventions are available at each stage. Think of it as a practical, phase-by-phase framework you can bring into your next session.
A Brief Grounding in Ego State Theory
Before we walk through the protocol, let’s get grounded in what we actually mean by ego states. The concept comes from John and Helen Watkins, who defined an ego state as "an organized system of behavior and experience whose elements are bound together by some common principle." In plainer terms: ego states are the different parts of ourselves that hold different feelings, memories, beliefs, and ways of responding to the world.
Here is the part that matters most for clinical work: everyone has ego states. They are a normal feature of personality organization, not something that only shows up in dissociative disorders. You have a professional self, a playful self, a version of you that comes out around your family of origin that might surprise your colleagues. That is ego state activity, and it is completely healthy when the boundaries between those states are flexible and permeable.
Trauma changes that equation. When a child experiences repeated harm, neglect, or threat, certain ego states develop rigid boundaries and take on protective roles. These maladaptive ego states were adaptive at the time. They kept the child safe, or as safe as possible. But in adult life and in the therapy room, they can create distressing symptoms, internal conflict, and therapeutic impasses that standard protocol alone may not resolve.
A quick distinction worth naming: ego states exist on a spectrum of dissociation. At one end, you have the normal, fluid shifting between parts of self that happens in everyday life. At the other end, you have the more rigid, dissociated alters seen in Dissociative Identity Disorder. Most of the ego state work EMDR clinicians encounter falls somewhere in the middle: protective parts, critical parts, child states, caretaker parts, and occasionally controlling or belligerent parts that formed under extreme conditions. Knowing where your client’s experience falls on that spectrum shapes everything about how you approach the work.
For a deeper exploration of the theoretical foundations of ego state therapy and how it has evolved over the past several decades, the 2020 literature review by Piedfort-Marin and colleagues is worth reading.
With this foundation in place, let’s look at how ego states show up across the EMDR protocol and what you can do about it at each phase.
Ego States Across the 8 Phases of EMDR
What follows is a phase-by-phase breakdown. For each phase, I have outlined what ego state activity typically looks like and what clinicians need in order to respond effectively. This is the practical core of the article, and it maps directly to how ego state therapy and EMDR work together in real clinical practice.
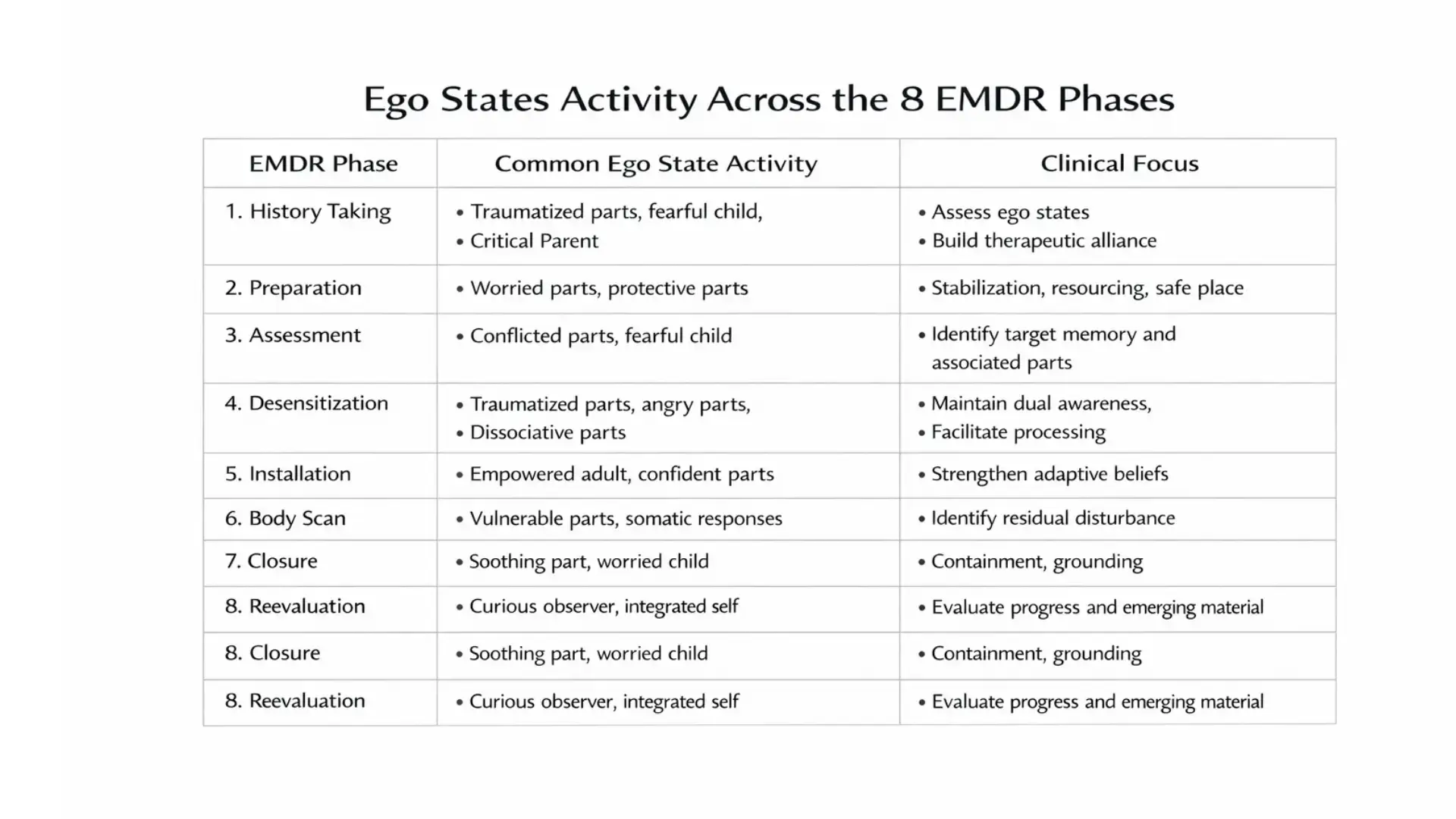
Phase 1: History Taking and Treatment Planning
What shows up: Gaps in narrative. Contradictory accounts of the same event told with total conviction each time. Sudden shifts in affect during intake that seem to come from nowhere. A client who is extraordinarily competent in professional settings but collapses in relational contexts. Protective parts steering the conversation away from certain topics, sometimes so subtly that you barely notice it happening.
What you need: Screening for dissociation is the starting point. Tools like the DES (Dissociative Experiences Scale) or the SDQ-20, or even a well-structured clinical interview, can help you identify the degree of ego state activity early. But beyond screening, the key clinical insight here is that history taking with complex trauma clients is itself an ego state process. Certain parts may hold memories that the presenting self cannot access or put into words. If you treat intake as simple data gathering, you will miss the parts of the story that the most activated ego states are carrying.
Key point: History taking is your first opportunity to notice which ego states are present, how they interact, and how rigid or permeable the boundaries between them are. What you learn here directly shapes your ego state informed EMDR treatment planning for everything that follows.
Phase 2: Preparation
This is the richest phase for ego state work in EMDR, and honestly, it is where the most common mistakes happen. Here is the scenario: you teach your client a calm place exercise. The adult self finds it helpful. But a child part inside that system has no idea what "calm" feels like, and a protective part interprets the whole exercise as a setup for something dangerous. The resource you just built works for one part of the system and is rejected or ignored by the rest.
What you need: Ego state-specific resourcing. Build resources for the parts, not just the presenting self. This is where techniques like Fraser’s Dissociative Table come in. It is a structured visualization for facilitating internal communication between parts, and it gives the ego state system a way to begin cooperating before you ever touch a target. Other EMDR Phase 2 ego state interventions include the Inner Sanctuary technique (building a felt sense of internal safety and communication), the Resource Room, and resourcing allies within the ego state system itself.
Key point: Phase 2 is where you establish internal cooperation. If parts do not feel included, informed, or safe, they will disrupt reprocessing later. Taking time here is not a delay. It is what makes the rest of the protocol possible. For clinicians working with C-PTSD presentations, EMDR and Complex PTSD with Erica Bonham covers extended Phase 1 and Phase 2 preparation in depth.
Phase 3: Assessment
What shows up: Target selection gets more complex when ego states are involved. The negative cognition may belong to one part ("I am powerless") while another part holds a completely different belief about the same event ("I caused it"). Your SUDS reading may reflect the distress of one state while another is numb or entirely unaware. The VOC may not resonate with the part that actually holds the trauma.
What you need: The ability to identify which ego state holds the target. Start asking questions like: Whose memory is this? Which part carries the distress? Which part would prefer this memory stay untouched? Treatment planning needs to account for the pattern exhibited by maladaptive ego states, not just the traumatic event on its own.
Key point: If you assess a target without knowing which part of the system holds it, your NC, PC, SUDS, and VOC may not accurately reflect the client’s internal experience. This disconnect is one of the most common reasons EMDR reprocessing stalls.
Phase 4: Desensitization
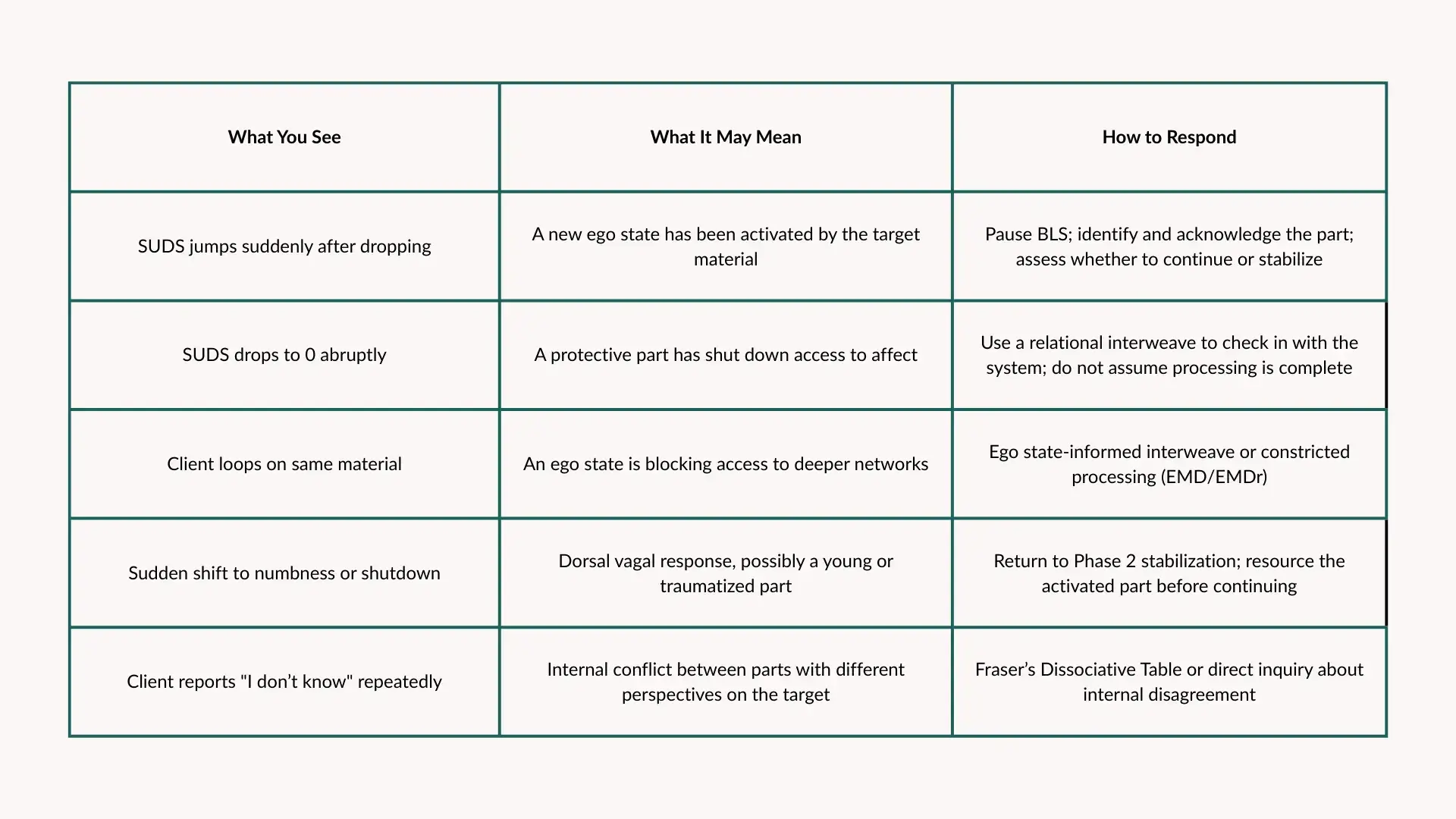
This is the phase where parts emerging during reprocessing becomes impossible to ignore. You will see sudden shifts in affect, from deep distress to flat numbness, or from engaged processing to complete shutdown. You will see looping, where the client circles the same material set after set without moving toward resolution. You will see SUDS that will not budge. And you may see a protective part step in and effectively block access to the target altogether.
What you need: Ego state-informed interweaves. When a protector part surfaces mid-set, the clinician needs to recognize it and respond appropriately. This might mean pausing bilateral stimulation to acknowledge the part directly, using a cognitive or relational interweave that addresses the part’s specific concern, or briefly returning to Phase 2 stabilization before continuing. For stuck processing specifically, Advanced EMDR Skills with Rebecca Kase covers interweave techniques, working-memory interventions, and constricted processing strategies (EMD and EMDr) that apply directly to these moments.
Key point: The presence of an ego state during desensitization is not a failure of the protocol. It is the protocol working correctly, revealing the internal system’s relationship to the trauma. The question is not whether parts will show up. They will. The question is whether you, the clinician, have the skills to respond when they do.
Phase 5: Installation
What shows up: The positive cognition may resonate beautifully with the adult self but feel foreign or even threatening to a child part. A protective part may reject the PC outright. "If I believe I’m safe now, I’ll let my guard down" is a perfectly logical concern for a part whose entire job has been vigilance. That resistance is not defiance. It is clinical information.
What you need: Check whether the PC is accepted across the ego state system, not just by the presenting self. If a part resists the positive cognition, that may signal incomplete processing or an ego state that has not yet been included in the work. Forcing installation over that resistance rarely ends well.
Phase 6: Body Scan
What shows up: Residual body sensations that belong to a specific ego state rather than to the target as a whole. A child part may hold tension, pain, or constriction in a location the adult self does not typically feel. The client might say something like, "My stomach hurts but I don’t know why," and the "why" is that a part of them is still holding something the rest of the system has processed.
What you need: Attunement. Is the body response coming from the presenting self or from a part? If a sensation arises that does not match the client’s current state, it may indicate an ego state that still needs attention before you move to closure.
Phase 7: Closure
What shows up: A client leaves the session feeling settled while a part remains activated internally. Between-session disturbance is common when ego states were touched during processing but not fully stabilized before session’s end. The presenting self reports feeling fine. Then the client calls two days later in distress because a part that was activated during processing never got contained.
What you need: Closure that addresses the whole system. Rebecca Kase’s "Tucking In" technique is designed specifically for this: helping each part that was activated during the session feel contained and cared for before the client walks out the door. Standard containment exercises that work for the adult self may not reach the parts that were stirred up during processing. This is one of the most practical and immediately applicable interventions covered in Ego States Integration for the EMDR Therapist.
Phase 8: Re-evaluation
What shows up: New material surfacing between sessions that belongs to an ego state not yet addressed in treatment. Shifts in the internal system’s dynamics. A previously guarded protective part may soften. A new part may emerge now that the system feels safer. The client’s relationship to their own internal experience begins to change.
What you need: A framework for tracking integration over time. Re-evaluation with ego states means checking in not just with the client’s presenting self but with the system as a whole. Are parts more cooperative? Are boundaries more flexible? Is the client reporting more internal coherence, less internal conflict, fewer moments of feeling "taken over" by a part? These are the markers of progress.
Key point: Integration is the long game. Phase 8 is where you assess whether the ego state work done across Phases 1 through 7 is holding, and where the treatment plan may need adjustment. It is also where you get the clearest picture of what is working and what still needs attention.

Why Ego State Skills Are Not Optional for EMDR Clinicians
If you have read this far, you have probably recognized your own clinical experience in at least a few of these phase descriptions. That is because complex trauma clients are not the exception in most EMDR practices. They are a significant portion of the caseload. And complex trauma, by definition, involves ego state activity: parts that formed in response to repeated harm, neglect, or threat, and that continue to influence the client’s internal experience, relationships, and capacity for processing.
Ego states are not a separate modality bolted onto EMDR. As Forgash and Copeley argued in their foundational work on integrating EMDR and ego state treatment, ego state therapy is part of how the Adaptive Information Processing model works in clients with layered trauma histories. The AIP model assumes that the brain’s information processing system will move toward adaptive resolution given the right conditions. When ego states are present, those conditions include the internal system’s readiness, cooperation, and felt safety, not just the clinician’s technical execution of the protocol.
The clinical consequences of not having these skills are real: stalled processing that does not respond to standard interventions, re-traumatization when parts are activated but not stabilized, therapeutic rupture when a protective part feels overridden rather than included, and clinician burnout from sessions that feel like they are going in circles.
The fact that EMDRIA lists ego state and EMDR integration as an approved advanced training topic signals something the field has recognized for a while now: this is not an elective. It is core clinical knowledge for anyone doing EMDR with trauma populations.
For clinicians who want a broader foundation in dissociation as it relates to EMDR practice, or who are preparing for EMDR intensive sessions where these dynamics surface with even greater intensity, building ego state competency is the foundation everything else rests on.
Build Your Ego State Toolkit
Ego States Integration for the EMDR Therapist with Rebecca Kase, LCSW
Everything in this article, covered in depth and with practical interventions you can bring straight into session. This on-demand training walks you through ego state theory, hands-on techniques across all 8 phases, Fraser’s Dissociative Table, the Resource Room, the Inner Sanctuary technique, parts-based interweaves for reprocessing, the Tucking In technique for closure, and frameworks for tracking integration in Phase 8.
6 EMDRIA, ASWB, and NBCC CEs. Lifetime access. Learn at your own pace and return to the material whenever your caseload calls for it.
References
Forgash, C., & Copeley, M. (Eds.). (2007). Healing the heart of trauma and dissociation with EMDR and ego state therapy. Springer Publishing.
Forgash, C., & Knipe, J. (2012). Integrating EMDR and ego state treatment for clients with trauma disorders. Journal of EMDR Practice and Research, 6(3), 120–137. https://connect.springerpub.com/content/sgremdr/6/3/120
Piedfort-Marin, O., Tarquinio, C., & Dunezat, P. (2020). The concept of ego state: From historical background to future perspectives. European Journal of Trauma & Dissociation, 5(3), 100189. https://www.researchgate.net/publication/347059929
Shapiro, F. (2018). Eye movement desensitization and reprocessing: Basic principles, protocols, and procedures (3rd ed.). Guilford Press.
Watkins, H. H. (1993). Ego-state therapy: An overview. American Journal of Clinical Hypnosis, 35(4), 232–240. https://pubmed.ncbi.nlm.nih.gov/8480666/
Watkins, J. G., & Watkins, H. H. (1997). Ego states: Theory and therapy. W. W. Norton & Company.
Stay connected with fun info, news, promotions and updates!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.