Five Myths About Dissociative Identity Disorder Therapists Need to Stop Believing
Mar 06, 2026
Written By: Rebecca Kase, LSW
Read Time: 9 Minutes
When Your Training Didn't Cover This
Sarah's been talking about her week when something shifts mid-sentence. Her voice changes, softer, younger. She stops, looks around like she's seeing the room for the first time, and asks, "Where am I?"
Your heart rate kicks up. Only three minutes have passed, but Sarah insists she just "woke up" here. She doesn't remember driving to your office or starting the session. She calls herself by a different name.
And you freeze. Because graduate school never covered this.
Maybe you got one lecture on DID sandwiched between eating disorders and substance use. Maybe the subtext was clear: if you see this, refer it out.
Except now the client is in your office. The dissociation is real. And what you were taught, that DID is rare, extreme, and "for specialists only", might not be true.

Here's the gap: dissociation shows up constantly in complex trauma work, yet most EMDR and trauma therapists lack adequate training. We internalized that working with dissociation is risky, that engaging parts makes things worse, that EMDR is too dangerous.
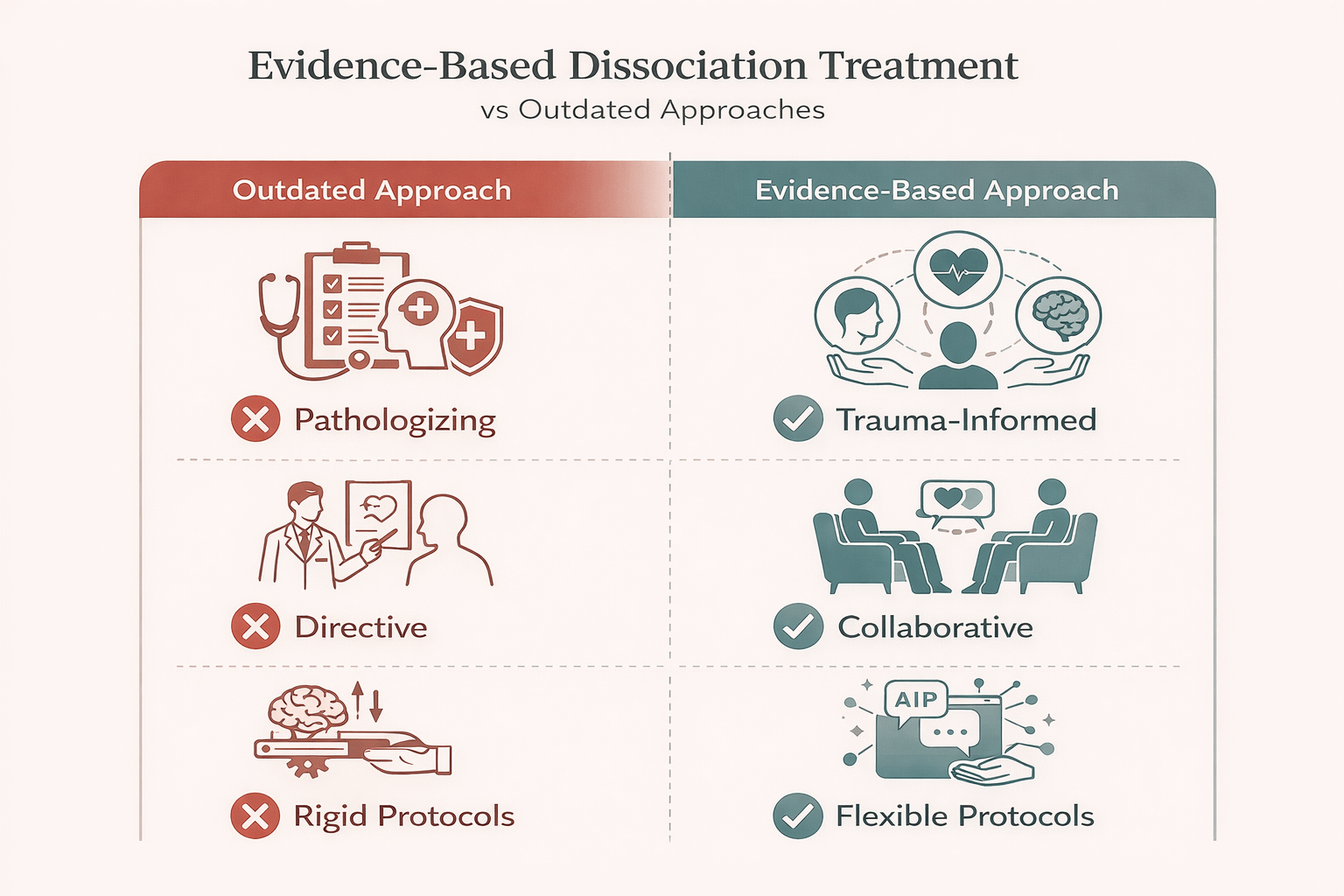
These beliefs aren't just outdated. They're actively harming treatment.
This article debunks five common myths about dissociative identity disorder and points you toward dissociation-informed EMDR and trauma therapist training that's ethical, practical, and actually accessible in the USA. Because the clients are already here. It's time to catch up.
Myth 1: "DID Is Rare and I'll Never See It"
You were probably taught that DID is vanishingly rare, maybe 0.01% of the population. Practically nonexistent.
Here's the reality: prevalence estimates range from 1-3% of the general population. That's roughly the same as bipolar disorder. Not common, but definitely not "you'll never see it" rare.
The kicker? Many DID and OSDD cases are consistently misdiagnosed as mood, psychotic, or personality disorders. You've probably seen it. You just didn't recognize it.
Think about clients who:
- Describe themselves in fragments ("part of me wants this, but another part refuses")
- Lose chunks of time regularly
- Show extreme shifts in presentation session to session
- Have early, severe trauma involving attachment figures
That's dissociation. Sometimes subclinical, sometimes a full disorder. All of it exists on a spectrum showing up constantly in complex trauma cases.
Your nervous system doesn't care about DSM criteria when surviving overwhelming threats. It fragments to protect you. For some, that fragmentation becomes persistent. For others, it's milder but clinically significant.
Every trauma and EMDR therapist needs foundational dissociation training, not just specialists. Dissociation isn't niche. It's core competency.
Myth 2: "Clients with DID Are Dangerous and Unpredictable"
This comes straight from Hollywood. The violent alter. The dangerous switch.
Let's be clear: people with DID are far more likely to be victims of violence than perpetrators. The sensationalized media portrayals bear almost no resemblance to clinical reality.
What you actually see: trauma survivors whose nervous systems learned to fragment as survival. People with internal conflict, yes. Struggles with trust and safety, absolutely. But not "dangerous" in the pop culture sense.
The instability you might observe - mood swings, self-harm, suicidal ideation -often improves when dissociation is recognized, validated, and treated with phase-oriented care. When therapists work with dissociative systems rather than pathologizing them, clients stabilize.
What makes DID clients seem "unpredictable"? They're responding to internal dynamics you can't see. Different parts hold different beliefs, emotions, and memories. When activated, the presentation shifts rapidly. That's not danger. That's information.
Dissociation-informed EMDR training teaches you to track shifts, work with containment and pacing, and reduce risk through better assessment. You learn to spot flooding before it happens, negotiate about safe targets, and recognize that "unpredictable" often means "I don't have the framework yet."
Once you have the framework, the work becomes manageable.
Myth 3: "You Should Avoid Engaging Parts or You'll Make Things Worse"
This myth has done tremendous damage.
The fear: if you acknowledge parts, you'll "reinforce" them. Make the client more fragmented. Create parts that didn't exist. So pretend they're not there and hope dissociation resolves on its own.
Except it doesn't work that way.
The parts already exist. Pretending they don't doesn't make them disappear. It communicates that a core piece of the client's experience is unacceptable. It creates shame and reinforces that their survival strategy is wrong.
The evidence is clear: structured engagement with parts reduces fragmentation over time. When you work collaboratively with a dissociative system, honoring protective functions, facilitating internal communication, helping parts develop awareness of each other, the client becomes more integrated, not less.
Integration doesn't mean fusion. It means reducing internal conflict, increasing cooperation, and helping the system function as a team rather than warring factions.
Ethical dissociation work honors the client's own language. Some use IFS language. Some talk about "versions of me." Some have distinct names. Some describe shifting into different modes. All valid. Your job is to meet them where they are.
Myth 4: "EMDR Is Too Dangerous for Dissociative Clients"
I get it. You've heard the horror stories. The client who got flooded during bilateral stimulation and ended up in crisis. The person who started switching rapidly between parts mid-processing and couldn't ground afterward. The EMDR session that seemed to destabilize someone for weeks. These outcomes are real, and the concerns are valid. EMDR applied without adequate dissociation assessment or pacing can absolutely cause harm. But the conclusion isn't "don't do EMDR with dissociative clients." It's "do dissociation-informed EMDR."
The principle is simple: assessment before activation. Before you reprocess anything, you need to know what you're dealing with. Is this client in their window of tolerance? Do they have adequate affect regulation skills? Is there internal agreement about working on this target, or are protective parts going to shut things down mid-session?
Dissociation-sensitive EMDR modifies all eight phases, not just Phase 4. Here's what that looks like:
Phase 1 (History Taking): You're not just mapping trauma. You're mapping the dissociative system. Who holds what memories? Which parts show up in daily life? What are the internal conflicts or protective functions?
Phase 2 (Preparation): You're building resources for the whole system, not just the presenting part. You're teaching grounding that works for hypoarousal, not just hyperarousal. You're establishing internal communication and safety agreements.
Phase 3 (Assessment): You're checking for internal consensus. Does the part holding this memory feel ready to work on it? Are protective parts on board, or will they sabotage the process?
Phase 4 (Desensitization): You're using titrated bilateral stimulation, slower, shorter sets, more frequent check-ins. You're watching for dissociative drift and adjusting in real time. You're using interweaves tailored to parts and states, not generic ones.Phases 5-8: Same adaptations. You're tracking which parts are present, facilitating internal communication, and ensuring that integration happens at the system level, not just within one part.When done well, EMDR with dissociative clients works beautifully. But "done well" requires training that most of us never got.
Myth 5: "If I Can't 'Fully Integrate' the System, I'm Failing"
Let's talk about goals.
There's a persistent assumption in dissociation treatment that full structural integration, meaning all parts fuse into one unified self, must always be the outcome. If you're not working toward that, you're doing it wrong. If the client doesn't achieve it, treatment failed.
This belief comes from older models of dissociation treatment and a fundamental misunderstanding of what clients actually want and need.
Many clients with DID prioritize functionality, safety, and cooperation among parts over fusion. They describe their parts as a team, a family, or a community. The goal isn't to eliminate everyone and become one person. It's to reduce internal conflict, improve communication, and function well in the world.
Lived experience and emerging literature emphasize client-defined goals, reduced internal conflict, and stigma-free language. Some clients do choose fusion as their end goal. Others don't. Both are valid.
Your job as a therapist isn't to impose a one-size-fits-all outcome. It's to help the client clarify what they actually want, work within their goals, and support their autonomy in making that choice.
This is where phenomenology and client narratives become essential. When you listen to how people with DID describe their own experience, how they conceptualize their parts, what integration means to them, what "healing" looks like in their life, you realize that the clinical models don't always match reality.
Courses like Clinical Competencies in Treating Dissociative Identities help therapists use phenomenology, client narratives, and research to craft realistic, ethical treatment plans within their actual scope. You're not trying to become the world's foremost DID expert. You're trying to work competently with the presentations you're already seeing.
And sometimes, competence means recognizing that a cooperative, functional system is success, even if it doesn't look like textbook "integration."
Why Specialized Dissociation Training Matters Now
Here's the bottom line: dissociation-informed training helps you do three things better.
- Accurate assessment. You stop confusing dissociation with resistance, inattention, or emotional dysregulation. You recognize the signs early and adjust your approach accordingly.
- Clearer case conceptualization. You understand the internal system, the protective structure, and the function of each part. You make treatment decisions based on that understanding, not on fear or outdated models.
- Safer trauma processing. Whether you're using EMDR, somatic work, or talk therapy, you know how to pace, titrate, and adapt for dissociative presentations. You reduce the risk of flooding, destabilization, and therapeutic ruptures.
We chose to bring Dr. Jamie Marich's Clinical Competencies training to TTI because it's exactly what I wish I'd had as a trauma therapist encountering dissociation in my practice. Jamie combines rigorous clinical expertise with her own lived experience of dissociation, which creates the kind of stigma-free, deeply humanizing training that helps therapists hold complexity without fear. USA-based EMDR and trauma clinicians now have access to high-quality, evidence-based dissociation training that fits their schedules, meets CE requirements, and doesn't require year-long commitments or travel. This is the practical, shame-free learning our field desperately needs.
Your Next Step as an EMDR or Trauma Therapist
So here's the question: which myth shows up most in your own training history, supervision, or internal dialogue?
Is it the "I'll never see this" myth that lets you avoid learning about dissociation? The "too dangerous" myth that keeps you from offering EMDR to clients who could benefit? The "avoid parts" myth that prevents you from working with what's actually happening in the room?
Whatever it is, there's a path forward.
Dissociation EMDR therapist training in the USA is more accessible than ever. The Clinical Competencies in Treating Dissociative Identities training offers practical, evidence-based skills for working with dissociation across the spectrum from subclinical presentations to full DID. You'll learn assessment, adaptation, and ethical treatment planning. You'll get continuing education credits. You'll join a community of trauma therapists doing this work.
This isn't about becoming a specialist. It's about building core competencies that should have been part of your original training but weren't.
Add dissociation-focused EMDR consultation and coursework to your 12-month learning plan. Register for training that bridges science and lived experience. Start challenging the myths you absorbed in graduate school and recognize that the field has moved forward and you can too.
The clients with dissociative presentations are already in your office. They're waiting for you to have the skills to help them. This is your chance to close the gap.
Frequently Asked Questions About DID and Dissociation Training
Is dissociation always a sign of a dissociative disorder like DID?
No. Dissociation exists on a spectrum. Many people experience clinically significant dissociative symptoms, depersonalization, time loss, identity disturbance without meeting full criteria for DID or OSDD. These presentations are common in complex PTSD and other trauma-related conditions. However, dissociative disorders are more prevalent than most therapists were taught, affecting 1-3% of the population, which is comparable to other serious mental health conditions.
Can EMDR be used safely with clients who dissociate?
Yes, when therapists have adequate dissociation training and modify their approach. EMDR can be highly effective for dissociative clients when you conduct thorough assessments, adjust pacing and bilateral stimulation, work collaboratively with parts, and prioritize stabilization. What's unsafe is applying standard EMDR protocols without recognizing or adapting for dissociation. Specialized training teaches you how to make these modifications effectively.
How do I know when I need specialized dissociation therapist training?
If you regularly encounter clients who "check out" in session, lose time, describe themselves in fragmented ways, or show rapid shifts in presentation, you need dissociation training. If you're uncertain about scope when DID is suspected, or if you avoid using EMDR with certain clients because you're worried about destabilization, that's a clear signal.
Formal training gives you the assessment and intervention skills to work confidently within appropriate boundaries.
Ready to move beyond the myths? The Clinical Competencies in Treating Dissociative Identities training gives trauma and EMDR therapists practical, science-backed tools for working with dissociation. Learn from experts who combine clinical expertise with lived experience, earn continuing education credits, and join a community of therapists building these essential competencies. Registration is open now.
References
Advanced Certificate in Dissociation Studies for EMDR Therapists. (2021, December 14). The Institute for Creative Mindfulness. https://www.instituteforcreativemindfulness.com/advanced-certificate-in-dissociation/
Greene, J., Graham, J., Gulnora Hundley, Zeligman, M., Bloom, Z., & Ayres, K. (2018). Counseling Clients with Dissociative Identity Disorder: Experts Share their Experiences. Journal of Counselor Practice, 9(1), 39–63. https://doi.org/10.22229/zpe728029
International Society for the Study of Trauma and Dissociation. (2011). Guidelines for Treating Dissociative Identity Disorder in Adults, Third Revision. Journal of Trauma & Dissociation, 12(2), 115–187. https://doi.org/10.1080/15299732.2011.537247
Kédia, M. (2009). La dissociation : un concept central dans la compréhension du traumatisme. L’Évolution Psychiatrique, 74(4), 487–496. https://doi.org/10.1016/j.evopsy.2009.09.013
Subramanyam, A., Somaiya, M., Shankar, S., Nasirabadi, M., Shah, H., Paul, I., & Ghildiyal, R. (2020). Psychological Interventions for Dissociative disorders. Indian Journal of Psychiatry, 62(8), 280. https://doi.org/10.4103/psychiatry.indianjpsychiatry_777_19
Team, T. T. (2019). Clinical Competencies in Treating Dissociative Identities. Traumatherapistinstitute.com. https://www.traumatherapistinstitute.com/Clinical-Competencies-in-Treating-Dissociative-Identities-Bridging-Lived-Experience-and-Science-For-the-Trauma-Therapist
The Art and Science of EMDR. (2024, February 17). Dr. Jamie Marich on EMDR and Dissociation. YouTube. https://www.youtube.com/watch?v=6vcto4c3Pwo
Stay connected with fun info, news, promotions and updates!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.