
trauma
ocd
ptsd

Stay in the loop
Trauma-informed tools, new trainings, and the occasional pep talk. No spam, ever.

Reading Time: 10 minutes
Therapists are vetted constantly. By clients who ask whether a modality has research behind it. By supervisors who want to see treatment plans grounded in evidence. By insurance companies, by licensing boards, by colleagues. And, more often than anyone admits out loud, by the therapist themselves, in the quiet moments between sessions, wondering whether what they are offering is actually doing what it is supposed to do.
Adding a new modality to your practice is a real investment. Time, money, supervision, the slow process of building enough competence that you can actually use the new approach in the room rather than just describing it. Before any of that begins, the reasonable question is whether the evidence justifies the work. For Acceptance and Commitment Therapy (ACT), the answer is generally yes, with some specific qualifications that this post will walk through honestly.
ACT is one of the most extensively studied psychotherapies in the field. As of early 2026, over 1,000 randomized controlled trials have been published examining ACT across a wide range of populations and presentations. The Association for Contextual Behavioral Science maintains a public index of meta-analyses and systematic reviews on the ACT evidence base, which currently includes well over a hundred such reviews.
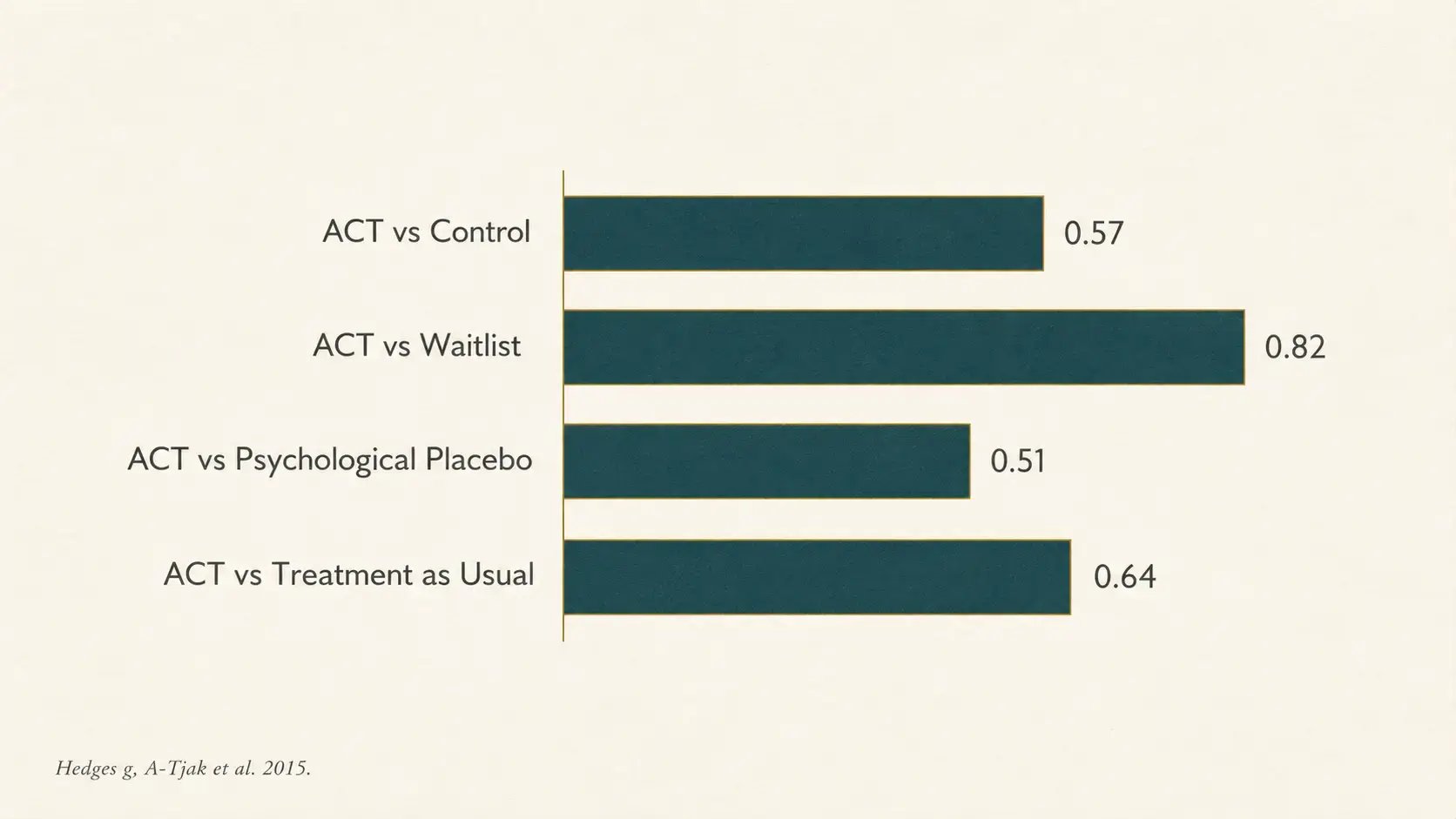
The two most-cited contemporary summaries of the ACT evidence are A-Tjak and colleagues (2015), which pooled 39 RCTs across 1,821 participants and reported a moderate overall effect size (Hedges' g = 0.57) for ACT against control conditions, and Gloster and colleagues (2020), which reviewed 20 meta-analyses covering 100 controlled effect sizes and over 12,000 participants. The Gloster review concluded that ACT was efficacious for all conditions examined, including anxiety, depression, substance use, pain, and transdiagnostic groups, and was generally superior to inactive controls, treatment as usual, and most active interventions other than CBT.
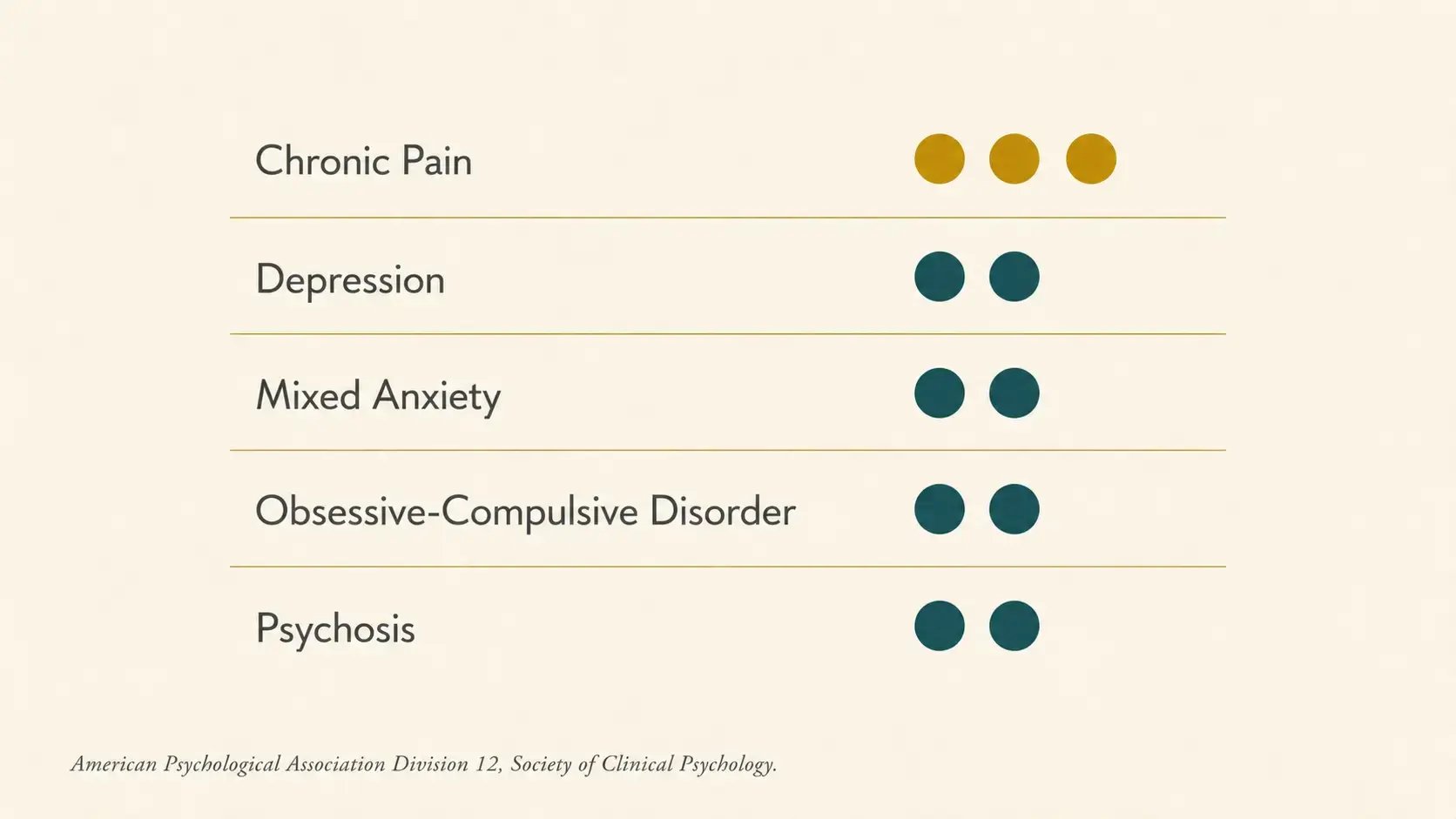
ACT is recognized by the American Psychological Association Division 12 (Society of Clinical Psychology) as an empirically supported treatment for chronic pain (strong research support) and as having modest research support for depression, mixed anxiety, OCD, and psychosis. The Substance Abuse and Mental Health Services Administration also lists ACT as empirically supported for OCD, depression, general mental health, and rehospitalization in its national registry.
This is where the evidence picture deserves the most careful honesty. ACT has not been shown to be superior to gold-standard PTSD treatments like prolonged exposure or cognitive processing therapy, both of which are first-line trauma-focused interventions with decades of accumulated evidence. The most recent VA trial directly comparing prolonged exposure to cognitive processing therapy found small differences in favor of PE, but with meaningful PTSD improvement in both groups. Neither was ACT.
That said, the trauma-specific ACT research base has grown substantially, and recent reviews are encouraging. A 2026 systematic review and meta-analysis by Rehman and colleagues, published in the Journal of Loss and Trauma, examined 25 studies on ACT for PTSD, including 20 in meta-analysis, and reported a mean effect size of 1.274 (95% CI 0.906 to 1.643). That is a large effect, though the authors note methodological variability across the included studies. The review concluded that ACT is associated with substantial improvements in psychological flexibility and reductions in PTSD symptoms.
An earlier Frontiers in Psychiatry review concluded that acceptance-based interventions are particularly well-suited to trauma populations because they directly target experiential avoidance, dissociation, and the shame, guilt, and disgust that frequently co-occur with PTSD. The review emphasized that ACT can promote neural and behavioral changes in trauma-related disorders even when used as an adjunctive rather than a primary treatment.
The most accurate framing of where the evidence currently stands is this: ACT is not the first-line treatment for PTSD, and it is increasingly supported as effective for PTSD symptoms and as a useful adjunct to or substitute for first-line trauma treatments when those are unavailable, unsuitable, or have left residual suffering that needs to be addressed. The clinical wisdom of using ACT alongside trauma processing has been ahead of the research, and the research is steadily catching up.
ACT has accumulating evidence for the treatment of PTSD, with recent meta-analyses reporting moderate to large effect sizes for symptom reduction. ACT is not currently listed by the American Psychological Association Division 12 as an empirically supported first-line treatment for PTSD in the same way that prolonged exposure, cognitive processing therapy, or EMDR are. The most current trauma-specific ACT review (Rehman et al., 2026) supports its use, with the caveat that more methodologically robust trials are needed.
The evidence for ACT in depression and anxiety is well-established. Multiple meta-analyses, including A-Tjak et al. (2015) and Gloster et al. (2020), have found ACT effective for both conditions and roughly equivalent to traditional CBT. The Gloster review reported that across head-to-head comparisons, ACT and CBT produced comparable outcomes for depression and anxiety, with neither approach showing consistent superiority.
This finding has been replicated enough times that the more interesting research question has shifted away from which approach is better and toward what mechanisms of change each one operates through. Some research suggests that ACT works primarily by increasing psychological flexibility, while CBT works primarily by changing cognitive content. Both can produce similar symptom outcomes through different routes, and the clinical implications for matching clients to approaches are still being worked out.
The chronic pain literature is the strongest part of the ACT evidence base. ACT was the first behavioral intervention to receive the APA Division 12 designation of strong research support for chronic pain (later revised to its current standing along with other conditions following methodological re-evaluations in the field). Multiple meta-analyses have demonstrated that ACT reduces pain interference, depression, and disability in chronic pain populations, with particularly strong effects on functional outcomes even when pain intensity itself does not change.
This matters for trauma clinicians because chronic pain populations and trauma populations overlap substantially. Clients with histories of trauma are at elevated risk for chronic pain conditions, and clients with chronic pain often carry unprocessed trauma. The clinical evidence supporting ACT for chronic pain is, indirectly, evidence supporting its use with a large segment of the trauma population.
Pulling the evidence together, ACT has the strongest research support in the following areas:
Chronic pain and chronic illness adjustment. Strong, well-replicated evidence across multiple meta-analyses.
Depression and anxiety disorders. Strong evidence, with effects comparable to traditional CBT.
Process-based mechanisms. Increasing psychological flexibility, reducing experiential avoidance, and clarifying values consistently emerge as mediators of treatment outcome.
Transdiagnostic and comorbid presentations. ACT performs well in mixed clinical populations, which is one of its distinctive strengths relative to disorder-specific protocols.
Health-related quality of life. Across both mental and physical health applications, ACT shows particularly strong effects on functional outcomes and quality of life measures, often more so than on symptom severity alone.
Honest accounting of the evidence requires naming where the gaps still are.
Trauma-specific ACT protocols. While the trauma-specific evidence has grown, the field is still in a relatively early stage of developing standardized ACT protocols for PTSD and complex PTSD. Most published studies use ACT in adjunctive or modified forms rather than as a standalone first-line treatment.
Complex PTSD. Research on ACT for the dissociative and structural complexity of C-PTSD is even earlier than the PTSD literature. Clinical wisdom suggests ACT skills like defusion, present-moment awareness, and self-as-context are useful for these clients. The empirical foundation for this is still being built.
Long-term outcomes and dosing. Most ACT trials report short to medium follow-up periods. Less is known about the durability of treatment gains over multi-year horizons, and the optimal dose of ACT for different conditions remains an open question.
Cultural and contextual factors. The majority of ACT research has been conducted in Western, English-speaking, and academic medical settings. Research on ACT in non-Western cultural contexts, in community mental health settings, and with historically underrepresented populations is growing but still limited.
None of these gaps undermines the case for ACT. They are the normal frontier of a maturing evidence base, and they are worth knowing because they shape what the modality can responsibly claim.
Research evidence is what justifies an investment in training. It is not what makes a modality work in the room. The bridge between the two is clinical skill, which only develops through structured training, deliberate practice, and supervision.
If the evidence summarized in this post has earned your interest, the next step is a training that translates the research into clinical practice. Our 1-Day Fundamentals Course for Trauma Clinicians with Jennifer Caspari, PhD, walks through the six core processes, the named clinical interventions that operationalize them, and the specific application of ACT to trauma work.
Jennifer is a clinical psychologist whose own practice is grounded in the evidence described here and in the lived experience of working with clients for whom ACT has been the modality that finally reached the suffering trauma processing alone did not.
The research will keep evolving. The clinical work will keep asking more of us. The training is where those two threads meet.
A-Tjak, J. G. L., Davis, M. L., Morina, N., Powers, M. B., Smits, J. A. J., & Emmelkamp, P. M. G. (2015). A meta-analysis of the efficacy of acceptance and commitment therapy for clinically relevant mental and physical health problems. Psychotherapy and Psychosomatics, 84(1), 30-36. https://doi.org/10.1159/000365764
Dindo, L., Van Liew, J. R., & Arch, J. J. (2017). Acceptance and commitment therapy: A transdiagnostic behavioral intervention for mental health and medical conditions. Neurotherapeutics, 14(3), 546-553. https://doi.org/10.1007/s13311-017-0521-3
Gloster, A. T., Walder, N., Levin, M. E., Twohig, M. P., & Karekla, M. (2020). The empirical status of acceptance and commitment therapy: A review of meta-analyses. Journal of Contextual Behavioral Science, 18, 181-192. https://doi.org/10.1016/j.jcbs.2020.09.009
Mendes, A. L., & Castilho, P. (2022). The emerging role of acceptance and commitment therapy as a way to treat trauma and stressor-related disorders. Frontiers in Psychology. https://pmc.ncbi.nlm.nih.gov/articles/PMC8771204/
Rehman, S., Ghazali, S. R., & Elklit, A. (2026). A systematic and meta-analytical review of Acceptance and Commitment Therapy for PTSD. Journal of Loss and Trauma, 31(1), 90-119. https://doi.org/10.1080/15325024.2025.2565354
Schnurr, P. P., Chard, K. M., Ruzek, J. I., et al. (2022). Comparison of prolonged exposure vs cognitive processing therapy for treatment of posttraumatic stress disorder among US veterans: A randomized clinical trial. JAMA Network Open, 5(1), e2136921. https://doi.org/10.1001/jamanetworkopen.2021.36921
