
Clinical Skills
ACT

Stay in the loop
Trauma-informed tools, new trainings, and the occasional pep talk. No spam, ever.

Read Time 14 Minutes
The question of why some therapy practices feel sustainable and others quietly deplete the clinician running them tends to be addressed at the level of individual variables: pricing, marketing, caseload size, work-life balance. These variables are real and they matter. The challenge with engaging them one at a time is that they are not actually one at a time in the lived experience of running a practice. They interact, they compound, and they tend to produce structural outcomes that no individual variable can predict on its own. A clinician with strong clinical skills but a weak business structure will stagnate. A clinician with excellent systems but unclear relational boundaries will erode the trust the practice depends on. Personal sustainability without the rest tends to produce a well-rested clinician whose practice is collapsing around them.
This piece offers a framework for thinking about therapy practice sustainability that integrates these variables rather than treating them in isolation. The four-pillar model described here is the diagnostic lens used in TTI's Practice by Design series, and it operates as a structured way to identify where a practice is currently strong, where it is leaking, and what the most useful next investment of attention is likely to be. The framework is not prescriptive about what a practice should look like in any specific way. It is descriptive about the structural conditions under which clinical practice tends to hold over the long arc of a career.
Most clinicians who experience their practice as unsustainable are not failing for lack of effort. They are usually working extraordinarily hard, often harder than the practice structurally requires, in ways that compound across years into the kind of depletion that does not resolve with time off. The diagnostic question that tends to be more useful than how hard the clinician is working is what the clinician is working on, and whether the underlying structure of the practice is calibrated to hold what the clinician is bringing to it.
A framework helps with this kind of diagnostic work in two ways. The first is by making the structural conditions of the practice visible as discrete elements that can be examined, rather than as a single overwhelming whole that resists analysis. The second is by clarifying the relationships between elements, so that a clinician working on pricing without also addressing operational systems, or addressing operational systems without examining clinical scope, can see why their effort is not producing the durability they expected. Practice sustainability is a systems outcome, and systems outcomes respond to systems analysis.
The four pillars described here function as that systems analysis. Each pillar carries distinct responsibilities, distinct failure modes, and distinct kinds of investment. They also interact in specific ways, which means that a weakness in one pillar tends to produce visible symptoms in the others. Understanding the full structure makes the source of the symptoms more identifiable than examining the symptoms alone.
Clinical integrity is the foundation pillar and the one most clinicians have invested in most deeply through their training and ongoing professional development. It refers to the depth and currency of the clinician's clinical skill, the honesty of their scope of practice, and the ongoing commitment to producing the quality of clinical work the practice represents itself as offering. Clinical integrity is not a static credential. It is a living commitment that requires continuous investment in continuing education, supervision, consultation, and the kind of reflective practice that allows a clinician to remain attuned to where their skill is strong and where it has limits. The research on therapist effectiveness consistently points to ongoing professional development as a contributor to sustained clinical outcomes over a career.
What this pillar looks like when it is strong: The clinician has a clear and defensible scope of practice, defined by the populations and presentations where their training and experience support competent clinical work. They invest deliberately in continuing education within that scope, with the kind of focused engagement that produces depth rather than breadth. They have meaningful supervision or consultation relationships, even later in their career, and they are willing to refer cases that fall outside their scope to colleagues whose training is better suited. Trust, both clinically and reputationally, follows naturally from this kind of grounded engagement with the work.
What this pillar looks like when it is leaking: Scope creep is one of the more common patterns: the clinician accepts cases outside their actual training because the income is needed or because saying no feels uncomfortable. Continuing education becomes scattered rather than deepening, with the clinician chasing the latest modality or specialization without consolidating around any of them. Supervision or consultation falls away after early career, sometimes for budget reasons and sometimes because the clinician believes they no longer need it. Clinical decisions begin to be made under fatigue or financial pressure rather than under clear judgment. The work continues, but the depth that defined it earlier begins to thin.

Relational clarity refers to the explicit definition and consistent maintenance of the relationships through which the practice operates: with clients, with referral sources, with consultees or supervisees if applicable, and with the clinician themselves about what they are actually offering and to whom. This pillar tends to be the one most clinicians assume is automatic, on the grounds that clinical training emphasizes relational competence as the core of the work. The assumption tends not to survive contact with the operational realities of running a practice, where the relational ambiguities are different in kind from the ones clinical training addresses.
What this pillar looks like when it is strong: Roles, expectations, and policies are defined from the start of every clinical relationship and revisited as needed throughout. Communication practices around scheduling, fees, cancellations, between-session contact, and the broader logistics of the work are stated explicitly and held consistently. Boundaries are not just announced but actually maintained, with the clinician's own behavior reflecting the standards they have set rather than drifting from them under pressure. Repair happens when ruptures occur, including the small ruptures around scheduling or payment that often go unaddressed in clinically-focused practices.
What this pillar looks like when it is leaking: The clinician finds themselves regularly accommodating requests that fall outside the structure they intended to maintain, often without quite registering the cumulative effect. Late cancellations are not charged when they should be. Between-session communication expands beyond what the practice can sustainably support. Fee discussions are deferred or hedged. Conversations with referral sources are unclear about scope, which produces poor-fit referrals that take longer to redirect than they would have to address directly upfront. The clinician begins to experience their own practice as somehow happening to them rather than being designed by them, which is often the first signal that this pillar needs attention.
Business structure refers to the operational infrastructure of the practice: the pricing model, the offer design, the scheduling and billing systems, the financial tracking, the marketing and visibility practices, and the various smaller decisions that collectively determine whether the practice runs on the clinician's continuous attention or on systems that hold the work without requiring continuous management. This is the pillar most clinicians have invested in least, often with significant anxiety attached to engaging it. Many clinicians experience a meaningful gap between their clinical sophistication and their operational sophistication, and the gap tends to widen across years of practice unless deliberately addressed.
What this pillar looks like when it is strong: The clinician knows their numbers. They have catalogued their annual practice overhead, calculated what the practice needs to generate in revenue to sustain them, and set their fees in conversation with that math. They have offers that are clearly defined: a specific articulation of what they provide, to whom, in what format, at what cost. They have systems that hold the operational work without requiring their continuous involvement, including automation of scheduling and billing, standardized intake processes, and explicit policies that reduce decision fatigue around the recurring administrative questions. They review their numbers, their systems, and their fees on a regular schedule, generally annually, which keeps the practice calibrated rather than drifting.
What this pillar looks like when it is leaking: Pricing is set by comparison rather than by calculation, and it has not been revisited in years. Practice overhead is uncatalogued and runs higher than the clinician realizes. Scheduling, billing, and administrative tasks consume hours per week that are not billable and not visible in the clinician's mental accounting of their work. Marketing happens reactively when caseload is low, rather than systematically. The financial structure of the practice is fragile in ways that are not obvious from the surface, which produces decision-making under pressure when ordinary disruptions occur. The clinician is often working harder than the practice structurally requires, without quite being able to identify why.
Personal sustainability refers to the clinician's own capacity, broadly understood as the energy, attention, emotional regulation, and physical resources available to do clinical work well over time. This pillar tends to be treated as the soft pillar, the one to address after the harder operational work is done. The framing is exactly backwards. A clinician whose personal capacity is already strained cannot build the other pillars effectively because the nervous system that is already dysregulated does not build elegant systems. It survives, which is a different mode of functioning than the deliberate design work the other pillars require. Recent research on burnout among mental health professionals has begun to document the downstream effects of unsustainable practice on clinical outcomes, which means personal sustainability has implications well beyond the clinician's individual wellbeing.
What this pillar looks like when it is strong: The clinician has an honest sense of how many clinical responsibilities they can sustainably hold, and they make caseload decisions in conversation with that capacity rather than against it. They have meaningful time off, not as an aspiration but as a built-in feature of the practice schedule. They invest in their own health, their relationships, and the parts of life outside clinical work that produce the resilience clinical work draws on. They recognize their energy and attention as finite resources to be allocated deliberately, rather than as raw inputs to be expended until empty. Their practice is designed for longevity rather than for maximum short-term output.
What this pillar looks like when it is leaking: The clinician chronically operates at the edge of their capacity, with little reserve for the inevitable demands that exceed the baseline. Time off is taken under duress rather than scheduled deliberately, and it often does not produce meaningful recovery because the underlying structural conditions remain unchanged. Self-care practices exist but are inconsistently maintained, and they tend to be the first thing to go when the practice gets busy. The clinician identifies as someone who runs hot, which is sometimes accurate as a description of temperament but more often a description of structural unsustainability that has been internalized as identity. The practice continues to function, but at a cost the clinician is paying personally and that compounds over years.
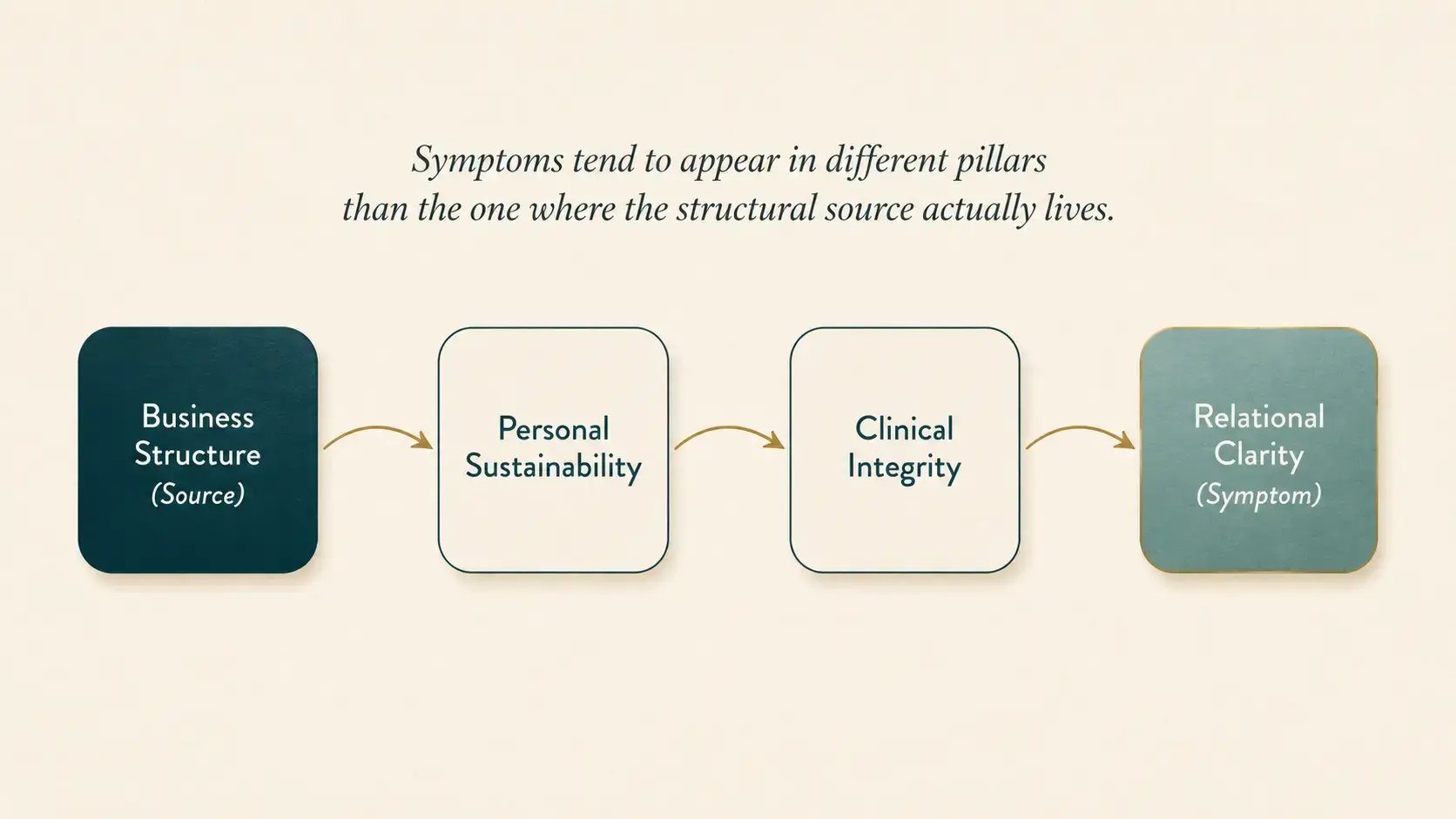
The four pillars do not function independently. A weakness in one tends to produce visible symptoms in the others, which is part of why diagnosing the actual source of practice fragility requires looking at all four rather than at the loudest one. A clinician whose business structure is weak (Pillar Three) tends to develop caseload pressure that erodes personal sustainability (Pillar Four), which over time degrades clinical integrity (Pillar One), which can produce the kind of low-grade relational drift that shows up as Pillar Two issues. The clinician experiencing this cascade often diagnoses the problem at the pillar where the symptoms are loudest, which is usually Pillar Four, and works on self-care without addressing Pillar Three, where the structural source actually lives.
Diagnostic honesty matters because the temptation to identify the leaking pillar as the one where the clinician already feels most competent tends to be substantial. A clinician who is clinically strong tends to attribute practice difficulties to factors other than clinical integrity, even when the actual issue is scope creep or insufficient continuing education investment. A clinician who has invested heavily in business systems tends to look elsewhere when the practice begins to feel fragile, even when the actual issue is a pricing structure that has not been recalibrated in years. The pillar where the clinician feels most comfortable is often where the most useful diagnostic work needs to happen, precisely because it is the place comfort has been protecting from honest examination.
A useful self-assessment process moves through each pillar in sequence, with a few honest questions designed to surface the actual state of the practice rather than the version the clinician carries in mental shorthand.
Clinical integrity: What does my actual scope of practice look like when I list the populations and presentations I see most often, and is that scope supported by my training? Where has my continuing education investment gone over the past three years, and what does that pattern reveal? Do I have meaningful supervision or consultation relationships, and am I willing to use them? When was the last time I turned down a case that fell outside my scope?
Relational clarity: Are my policies on cancellations, between-session contact, fees, and scheduling stated clearly and consistently held? Do my actions match the standards I articulate, or have they drifted under pressure? Are there clients or referral relationships where the ambiguity around expectations is producing friction I have been working around rather than addressing? Where is my own behavior teaching the people around me to expect more than the practice can sustainably provide?
Business structure: Do I know what my practice needs to earn to sustain me, calculated from desired take-home plus taxes plus overhead, divided by realistic billable hours? Is my fee actually calibrated to that number, or to comparison with other clinicians? What administrative tasks am I doing personally that could be systematized or delegated? When did I last review the actual annual cost of running my practice, and would I be surprised by the figure?
Personal sustainability: Am I operating with reserve, or at the edge of my capacity most weeks? Is the time off I take producing meaningful recovery, or returning me to the same depletion? Are the practices that sustain me outside clinical work consistently maintained, or are they the first thing to disappear when the practice gets busy? Would the structure of my practice still feel sustainable if my caseload reduced modestly, or is the current intensity the only configuration that holds the numbers together?
This framework was developed by Rebecca Kase, LCSW, founder and CEO of the Trauma Therapist Institute, in the course of her own clinical and entrepreneurial work. She recently wrote about the four pillars in a more personal register in her essay on Substack reflecting on what these pillars look like from inside the practice rather than at the systems level the present article describes. Her piece is a useful companion to the operational frame above, particularly for clinicians who want to understand the four pillars in the context of the personal experience of running a clinical practice over time. For the deeper reflective layer underneath the systems analysis, her essay on the four pillars is worth reading alongside this article.
What are the four pillars of a sustainable therapy practice? The four pillars are clinical integrity, relational clarity, business structure, and personal sustainability. Each addresses a distinct structural dimension of clinical practice. Clinical integrity is the depth of the clinical work itself. Relational clarity is the consistency of relationships and policies. Business structure is the operational infrastructure. Personal sustainability is the clinician's own capacity over time.
Why is structure more important than effort in private practice? Most clinicians who experience their practice as unsustainable are working extraordinarily hard, often harder than the structure requires. Sustainability is a systems outcome rather than an effort outcome, which means it responds to changes in the underlying structure of the practice rather than to additional effort within an unchanged structure. Effort without structure tends to produce burnout.
How do I assess which of the four pillars is weakest in my practice? Self-assessment is most useful when conducted with honesty about each pillar in sequence. The pillar that is most protected from honest examination, often the one the clinician feels most competent in, is frequently where the most productive diagnostic work needs to happen. Symptoms tend to appear in different pillars than the one where the structural source actually lives.
Can I work on just one pillar at a time? The pillars interact, which means significant investment in one tends to produce visible effects in the others. Working on one pillar deliberately, particularly the one where structural issues are most concentrated, is usually more effective than spreading attention thinly across all four. Most clinicians benefit from focused attention on one pillar at a time over a multi-month timeline.
How long does it take to build a sustainable practice using this framework? Most clinicians who use the four-pillar framework deliberately see meaningful structural shifts within twelve months, with deeper changes accumulating over two to three years. The work is rarely accomplished in a single sprint. It tends to be a year or more of deliberate attention to whichever pillar most needs it, with the structural conditions of the practice shifting incrementally rather than dramatically.
The most useful starting point in this work is rarely the pillar that feels most pressing in the moment. It is more often the pillar that has been protected from honest examination by virtue of feeling settled. A clinician who self-assesses across all four with appropriate honesty will usually identify one pillar where the assessment surfaces more than expected, and that pillar is generally the most productive place to start. The investment of attention at the actual source produces results that radiate outward into the other pillars, while attention at the loudest symptom often does not.
Building these pillars is rarely accomplished in a single sprint. It is more often a year of deliberate attention, sometimes longer for clinicians whose practices have drifted significantly from their intended design. The work is generally not glamorous in the moment, and it tends to produce results that compound across years rather than across weeks. The clinicians who do this work tend to describe their practice differently a year or two in than they did at the start, not because anything dramatic changed but because the structural conditions underneath the work shifted enough to produce a different daily experience of the practice as a whole.
|
Practice by Design: Building a Sustainable Therapy or Consultation Business is the four-hour workshop where Rebecca Kase, LCSW & CEO walks clinicians through the full four-pillar framework in a single focused session.
You leave with a written purpose statement, a completed Four Pillars assessment, a defined niche and offer, and a 90-day pilot plan you can begin executing when you log off.
Friday, July 31, 2026 at 10:00 AM Central. Live + recorded with lifetime access. $147.
|
|
Prefer to start with the self-paced version? The Business Accelerator Kit Download includes the Four Pillars self-assessment, the Hourly Math Worksheet, and the foundational worksheets that anchor the series. $29 with lifetime access.
|
Mullen, P. R., Backer, A., Chae, N., & Li, H. (2024). Effective burnout prevention strategies for counsellors and other therapists: A systematic review and meta-synthesis of qualitative studies. Counselling Psychology Quarterly. https://doi.org/10.1080/09515070.2024.2394767
Norcross, J. C., & Lambert, M. J. (2018). Psychotherapy relationships that work III. Psychotherapy, 55(4), 303-315. https://doi.org/10.1037/pst0000193
Yang, Y., & Hayes, J. A. (2020). Causes and consequences of burnout among mental health professionals: A practice-oriented review of recent empirical literature. Psychotherapy, 57(3), 426-436. https://doi.org/10.1037/pst0000317
