
Clinical Skills
ACT

Stay in the loop
Trauma-informed tools, new trainings, and the occasional pep talk. No spam, ever.

Read Time: 10 Minutes
There is a particular kind of discomfort that settles in when you are a good EMDR therapist working with a teenager who will not cooperate with the protocol. You know the phases. You have been through the training, sat through the consultation, watched the demo videos. The standard script has worked with dozens of adult clients. And now you are across from a sixteen year old who rolled her eyes at the safe place exercise, told you the SUD scale was "stupid," and responded to your careful "notice what comes up" prompt with a shrug and a muttered "I don’t know."
You are not doing EMDR wrong. You are doing it to the wrong kind of brain.
Adolescence is not a diminished version of adulthood. It is a distinct neurodevelopmental window with its own architecture, its own chemistry, and its own relationship to memory, emotion, and meaning. When the EMDR protocol meets that window without adaptation, it does not fail because the therapist is inexperienced. It fails because it was not built for the brain in the room.
The phrase the research literature keeps returning to is remodeling. Between roughly ages ten and twenty five, the adolescent brain undergoes a structural renovation that rivals the one that happens in the first few years of life. Synaptic pruning accelerates. Myelination continues well past the teenage years. Connectivity reorganizes. And it does not happen evenly.
Neuroscience research on myelin development using macromolecular proton fraction mapping has shown that cortical gray matter and white matter myelinate on different schedules through adolescence and late childhood, with the process continuing into the twenties in some regions (Corrigan et al., 2021). More recent work on personalized functional brain networks has mapped how the brain’s multi-scale organization shifts systematically through youth in ways that track neurocognitive development (Pines et al., 2022). The architecture is not just growing. It is reorganizing.
 This reorganization has a well-documented asymmetry. Subcortical regions involved in emotional reactivity and reward processing mature earlier than the prefrontal regions responsible for top-down regulation. Casey and Jones described this as an imbalance between functionally mature subcortical circuitry and a still-developing prefrontal cortex, an imbalance that accounts for the heightened sensitivity to reward, peer influence, and emotional intensity that characterizes adolescence (Casey & Jones, 2010). The car has a fully operational accelerator before it has fully operational brakes.
This reorganization has a well-documented asymmetry. Subcortical regions involved in emotional reactivity and reward processing mature earlier than the prefrontal regions responsible for top-down regulation. Casey and Jones described this as an imbalance between functionally mature subcortical circuitry and a still-developing prefrontal cortex, an imbalance that accounts for the heightened sensitivity to reward, peer influence, and emotional intensity that characterizes adolescence (Casey & Jones, 2010). The car has a fully operational accelerator before it has fully operational brakes.
This is not a character flaw or a phase to be endured. It is a design feature. The adolescent brain is wired to take risks, seek novelty, and form intense attachments outside the family of origin because those are the developmental tasks it is built for. Siegel calls it ESSENCE: emotional spark, social engagement, novelty seeking, and creative exploration. None of that is pathology. All of it is at odds with the standard EMDR protocol as it was originally designed.
The clinical translation is this. When you bring standard EMDR preparation into a room with a teen, you are asking a brain that is hyperaware of social evaluation to participate in an exercise that can feel transparently performative. You are asking a brain whose working memory is routinely taxed by school, social dynamics, and hormonal noise to hold a complicated dual-attention task. And you are asking a prefrontal cortex that is still years from full maturation to do the kind of top-down regulation that the protocol quietly assumes is already online.
The eye roll is not resistance. It is the correct response from a nervous system that has clocked the mismatch before you have.
Consider what happens with SUD scaling. In adult EMDR, asking a client to rate distress from zero to ten is a straightforward piece of structure. For a teen who spends most of her waking hours being evaluated on numerical scales, from test scores to Instagram metrics to the social standing she tracks through group chats, that same ask can land as another performance demand. Some teens produce a rating to comply. Others stall. Others simply leave the session. The scale was designed for precision. In adolescent clinical work, it often produces the opposite.
Consider what happens with "notice what comes up." The instruction assumes a client who can interocept, who has a ready vocabulary for internal states, and who trusts that reporting something imperfect or ugly will be met with curiosity rather than correction. Many adults struggle with all three. Many teens, particularly teens whose trauma histories involve caregivers who punished or dismissed their internal experience, struggle with all three and then some. The prompt invites self-disclosure that the brain in the room is not ready to offer.
Consider what happens with a full ninety minute reprocessing session. Research on trauma-focused treatment retention in adolescents consistently identifies premature termination as one of the field’s most significant clinical challenges. The standard session length, the standard pacing, the standard expectation of sustained attention to distressing material: each of these was calibrated for an adult nervous system with more stable executive function, not for a teenager whose working memory can be knocked offline by an incoming text.
None of this means EMDR does not work with adolescents. The evidence that it does is accumulating. A recent case series of twenty two adolescents with complex PTSD secondary to childhood abuse showed meaningful reductions in post-traumatic and associated symptoms following EMDR treatment, suggesting that when adapted appropriately, EMDR can be effective even in complex adolescent presentations (Rolling et al., 2024). The International Society for Traumatic Stress Studies includes EMDR in its treatment recommendations for children and adolescents with PTSD. The protocol has a place. It just needs translation.
This is the question that gets worked through in consultation rooms across the field. How far can you adapt EMDR for adolescents before you have left EMDR behind?
The answer most seasoned consultants land on is this: fidelity lives in the Adaptive Information Processing model, in the eight-phase structure, and in the clinical logic that links preparation to processing to integration. Fidelity does not live in the exact wording of the SUD scale, the specific imagery used in resourcing, or the expected length of a reprocessing set. Those are vehicles. The engine is the model.
This distinction matters because it frees clinicians from a false binary. You do not have to choose between running the protocol as written and abandoning EMDR. You can stay in the eight phases while using a concrete scaling tool instead of zero to ten. You can stay in AIP while replacing a guided visualization with a real physical space the teen already feels safe in. You can stay in fidelity while shortening processing exposures and building in containment breaks.
What you cannot do is skip preparation because a teen seems verbally fluent, skip target selection because he seems eager, or push through processing when working memory is visibly failing. Those shortcuts are where adolescent EMDR goes wrong, and they are usually the product of a clinician trying to make an adult protocol fit by moving faster rather than by adapting the design.
The following three are not the whole picture. They are starting points, the changes clinicians most often report as inflection points when they begin doing EMDR with teens in a developmentally grounded way.
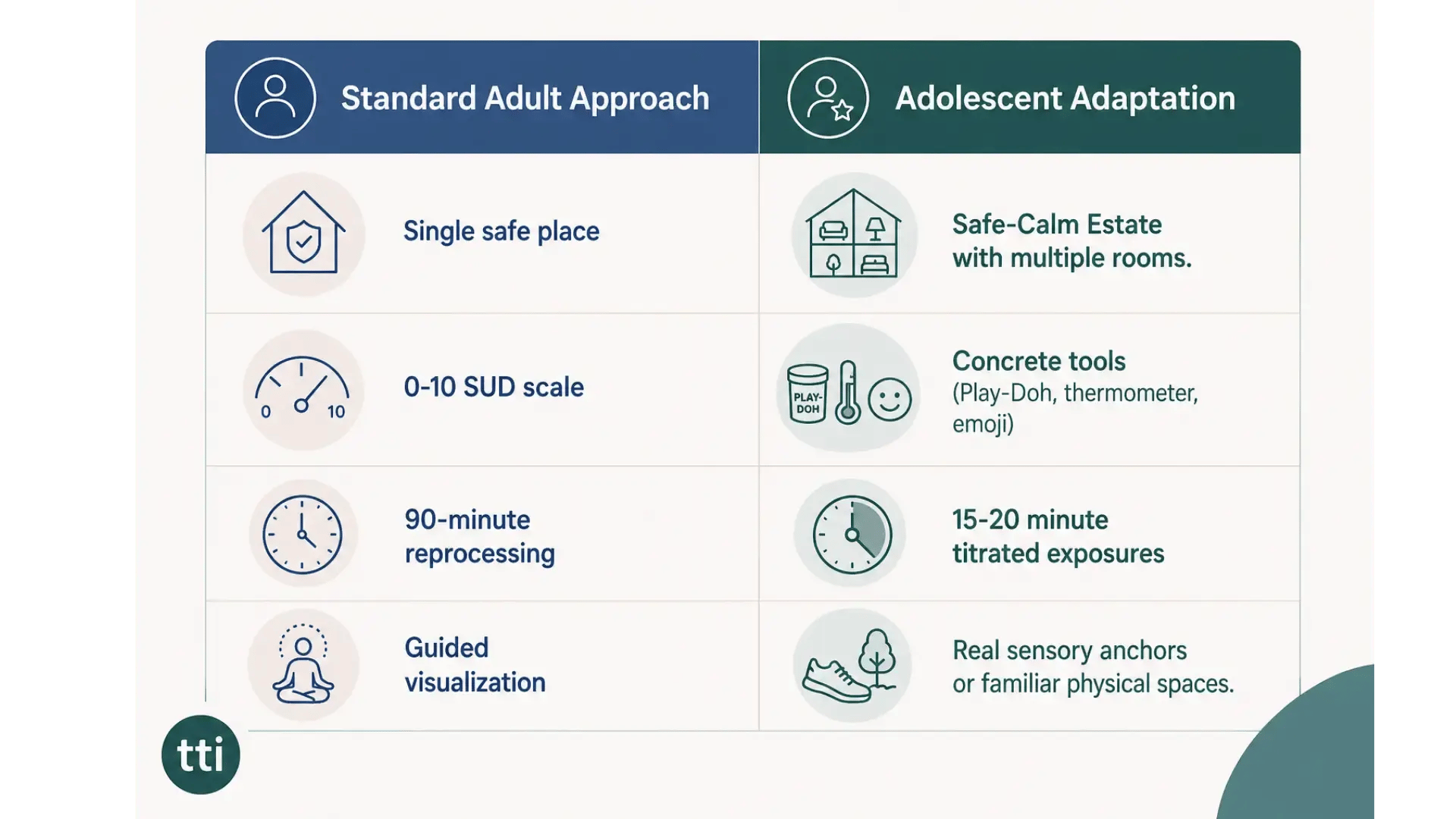
1. Build a Safe/Calm Estate, not a Safe Place
The traditional safe place exercise asks a client to imagine a single location that feels calming and then to anchor to it during distress. For adult clients, this often works. For adolescents, a single imagined place frequently feels thin, performative, or boring. The Safe/Calm Estate is an alternative that functions as a memory palace: a larger imagined space with multiple rooms, each holding a different resource. One room for comfort, one for boundary setting, one for a protector figure, one for a memory of strength. The estate can be drawn, mapped digitally, described in writing, or built inside a video game world the teen already knows.
The estate works because it matches how adolescent memory actually organizes itself. Teens already hold complex spatial and narrative worlds in their minds. Meeting them there, rather than asking them to invent something thinner, is the adaptation.
2. Replace abstract scales with concrete tools
Lumps of Play-Doh. A drawn thermometer. An emoji sequence the teen selects himself. A body outline she can mark on. Any of these can do the work of a SUD or VOC scale without triggering the test-taking anxiety that numerical scaling often activates. The principle is that measurement should be visible and tactile rather than abstract and evaluative.
This is a small change with an outsized effect. Clinicians who make it consistently report that teens engage with measurement for the first time, because it finally feels like something other than a quiz.
3. Shorten processing exposures and titrate aggressively
Adult protocol assumes sustained processing sets and a client who can hold dual attention across ninety minutes. Adolescent working memory often cannot. Shortened exposures, fifteen to twenty minutes of processing at a time with clear containment and regulation breaks in between, protect against the flooding and shutdown that derail so many teen sessions.
The titration techniques Jon Roberts teaches (the Walkie-Talkie approach, the Videotape technique) are specifically designed to keep a teenager’s working memory from crashing under the load of full reprocessing. They are not workarounds. They are developmentally appropriate applications of the same clinical logic that governs pacing with any complex trauma presentation.
One of the harder skills in adolescent EMDR is knowing when to stop moving forward. A teen can present as engaged and verbally fluent while her nervous system is quietly closing down. A teen can produce an articulate target while he is actively dissociating. A teen can report a SUD drop while none of the processing has actually integrated.
The markers to watch are not the ones clinicians are typically trained to track. Watch the body. Watch the eyes. Watch the pace of speech and the length of pauses. Watch what happens when you name something the teen has not named first. If the session starts moving faster than the nervous system in the room can handle, you have left the work. Slowing down is not a failure of the protocol. It is often the most faithful application of it.
 This is particularly true for adolescents with complex or developmental trauma, whose presentations frequently involve dissociation, parts fragmentation, and high-risk behaviors that function as both symptom and protection. When these elements are in the picture, the standard protocol almost always requires modification, and the decision to slow down or move back to preparation is a clinical skill in its own right. The same clinical reasoning applies to complex PTSD presentations in adults, and the underlying logic transfers well.
This is particularly true for adolescents with complex or developmental trauma, whose presentations frequently involve dissociation, parts fragmentation, and high-risk behaviors that function as both symptom and protection. When these elements are in the picture, the standard protocol almost always requires modification, and the decision to slow down or move back to preparation is a clinical skill in its own right. The same clinical reasoning applies to complex PTSD presentations in adults, and the underlying logic transfers well.
When it is working, adolescent EMDR looks less like a protocol and more like a collaboration. The teen has a vocabulary for her own parts. The clinician is not performing expertise; she is holding structure while remaining curious. Preparation is not a perfunctory box to check before the real work starts. It is the real work, for longer than the standard timeline suggests, until the nervous system in the room can actually hold what processing asks of it.
The teen starts showing up on time. The eye rolls soften. A parent reports something small has shifted at home. Processing, when it begins, moves in titrated increments that protect rather than push. And the teen, maybe for the first time, has an experience of therapy that does not ask her to perform maturity she has not yet developed. She gets to be exactly the brain she is, in the room, being helped.
Is EMDR safe for teenagers? The current evidence base supports EMDR as a treatment for adolescents with PTSD, with emerging research suggesting efficacy in complex PTSD presentations as well (Rolling et al., 2024). Safety depends on adequate preparation, developmental adaptation, and clinician training in adolescent-specific modifications. EMDR delivered without those modifications carries risks of dropout, flooding, and destabilization that can be avoided with appropriate clinical skill.
At what age can EMDR start? EMDR has been used with children as young as preschool age in adapted forms. The clinical question is rarely about a minimum age and more about whether the developmental adaptations match the client in the room. Different developmental windows call for different adaptations. Adolescent EMDR sits between child-focused and adult-focused work and requires its own specific framework.
Does EMDR work differently for teens with complex trauma? Yes. Complex, developmental, or chronic relational trauma tends to present in adolescents with layered parts, dissociation, and high-risk behaviors that the standard protocol is not designed to address directly. In these presentations, preparation is longer, target selection is more deliberate, and processing is frequently titrated. For teens whose presentations also involve substance use or self-harm, specialized protocols are often indicated alongside the standard eight phases.
The clinicians who do this work well are not the ones with the tightest adherence to the adult protocol. They are the ones who understand that fidelity to EMDR and fidelity to the adolescent in the room are the same thing, and that protecting both requires genuine developmental knowledge, not just protocol knowledge. That knowledge is teachable. It is what separates clinicians who dread teen clients from clinicians who have found something meaningful in the work.
For clinicians who want to deepen this work, it helps to have a framework specifically built for the adolescent brain: how neurodevelopment shapes case conceptualization, how preparation has to change, how parts work applies to teen presentations, and what to do when high-risk behaviors are part of the clinical picture. That framework is what transforms adolescent EMDR from a guessing game into a discipline.
EMDR with Adolescents: Parts Work, Modified Processing, and High-Risk Behaviors is a five-module on-demand training with Jon Roberts, LCSW, CAS.
Built around a continuous case study of a fifteen year old client, it walks clinicians through every adaptation that makes EMDR land with teens aged 13 to 18. 5 CEs (EMDRIA, ASWB ACE, NBCC). Available July 30, 2026.
I’m Ready to Work More Effectively With Teen Clients →
Casey, B. J., & Jones, R. M. (2010). Neurobiology of the adolescent brain and behavior: Implications for substance use disorders. Journal of the American Academy of Child & Adolescent Psychiatry, 49(12), 1189-1201. https://pmc.ncbi.nlm.nih.gov/articles/PMC3099425/
Corrigan, N. M., Yarnykh, V. L., Hippe, D. S., Owen, J. P., Huber, E., Zhao, T. C., & Kuhl, P. K. (2021). Myelin development in cerebral gray and white matter during adolescence and late childhood. NeuroImage, 227, 117678. https://pmc.ncbi.nlm.nih.gov/articles/PMC8214999/
International Society for Traumatic Stress Studies. (2020). ISTSS prevention and treatment guidelines. https://istss.org/clinical-resources/trauma-treatment/istss-prevention-and-treatment-guidelines/
Pines, A. R., Larsen, B., Cui, Z., Sydnor, V. J., Bertolero, M. A., Adebimpe, A., Alexander-Bloch, A. F., Davatzikos, C., Fair, D. A., Gur, R. C., Gur, R. E., Li, H., Milham, M. P., Moore, T. M., Murtha, K., Parkes, L., Thompson-Schill, S. L., Shanmugan, S., Shinohara, R. T., … Satterthwaite, T. D. (2022). Dissociable multi-scale patterns of development in personalized brain networks. Nature Communications, 13(1), 2647. https://www.nature.com/articles/s41467-022-30244-4
Rolling, J., Fath, M., Zanfonato, T., Durpoix, A., Mengin, A. C., & Schröder, C. M. (2024). EMDR–Teens–cPTSD: Efficacy of eye movement desensitization and reprocessing in adolescents with complex PTSD secondary to childhood abuse: A case series. Healthcare, 12(19), 1993. https://pmc.ncbi.nlm.nih.gov/articles/PMC11476079/
