
Professional Development
private practice
practice building

Stay in the loop
Trauma-informed tools, new trainings, and the occasional pep talk. No spam, ever.

Read Time 11 Minutes
Most EMDR training is, by necessity, protocol-focused. Clinicians learn the eight phases, the assessment script, the bilateral stimulation, the order of operations. What they often do not learn, at least not in any depth, is what is actually happening inside a teenager’s brain when trauma gets stored. That gap matters. It shapes every clinical decision a therapist makes with an adolescent client, even the decisions she does not realize she is making.
The teenager sitting across from you is not a smaller adult. Her brain is in the middle of a structural renovation that is unlike any other developmental period after infancy, and that renovation is happening at the same time she is processing trauma she may not be able to name. Understanding what is going on neurologically does not replace clinical skill. It calibrates it. The clinician who knows how memory is being laid down in an adolescent system makes different choices about pacing, preparation, and target selection than one who is running an adult protocol on a teenager and hoping for the best.
The adolescent brain undergoes structural changes between roughly ages ten and twenty-five that are second only to the rapid development of infancy. Two processes do most of the work. The first is synaptic pruning: the systematic elimination of neural connections that are not being used, sharpening efficiency in the connections that remain. The second is myelination: the wrapping of axons in fatty tissue that dramatically speeds up neural transmission. Together, these processes reorganize the brain from the inside out.
The reorganization is not uniform. Subcortical regions involved in emotion, reward, and threat detection mature earlier than the prefrontal cortex, which is responsible for top-down regulation and executive function. The result is what neuroscientists call a developmental imbalance: the gas pedal develops faster than the brake. Research on the integration of executive, memory, and mesolimbic systems shows that the developmental refinement of hippocampal-prefrontal interactions is what eventually allows adolescents to extract information from prior experience to support goal-oriented behavior, but this integration is still being built throughout the teenage years (Murty et al., 2016).
Daniel Siegel describes adolescence as a period of remodeling rather than a phase of immaturity to be endured, and the framing matters clinically. The teen brain is doing exactly what it is supposed to be doing: reshaping itself for the adaptive challenges of adulthood. Siegel’s framework for the adolescent brain identifies four core qualities that emerge during this period (Siegel, 2014). Each one shapes what teenagers need from therapy.
Siegel uses the acronym ESSENCE: Emotional Spark, Social Engagement, Novelty Seeking, and Creative Exploration. Each is a feature of healthy adolescent neurodevelopment. Each also has direct implications for clinical work.
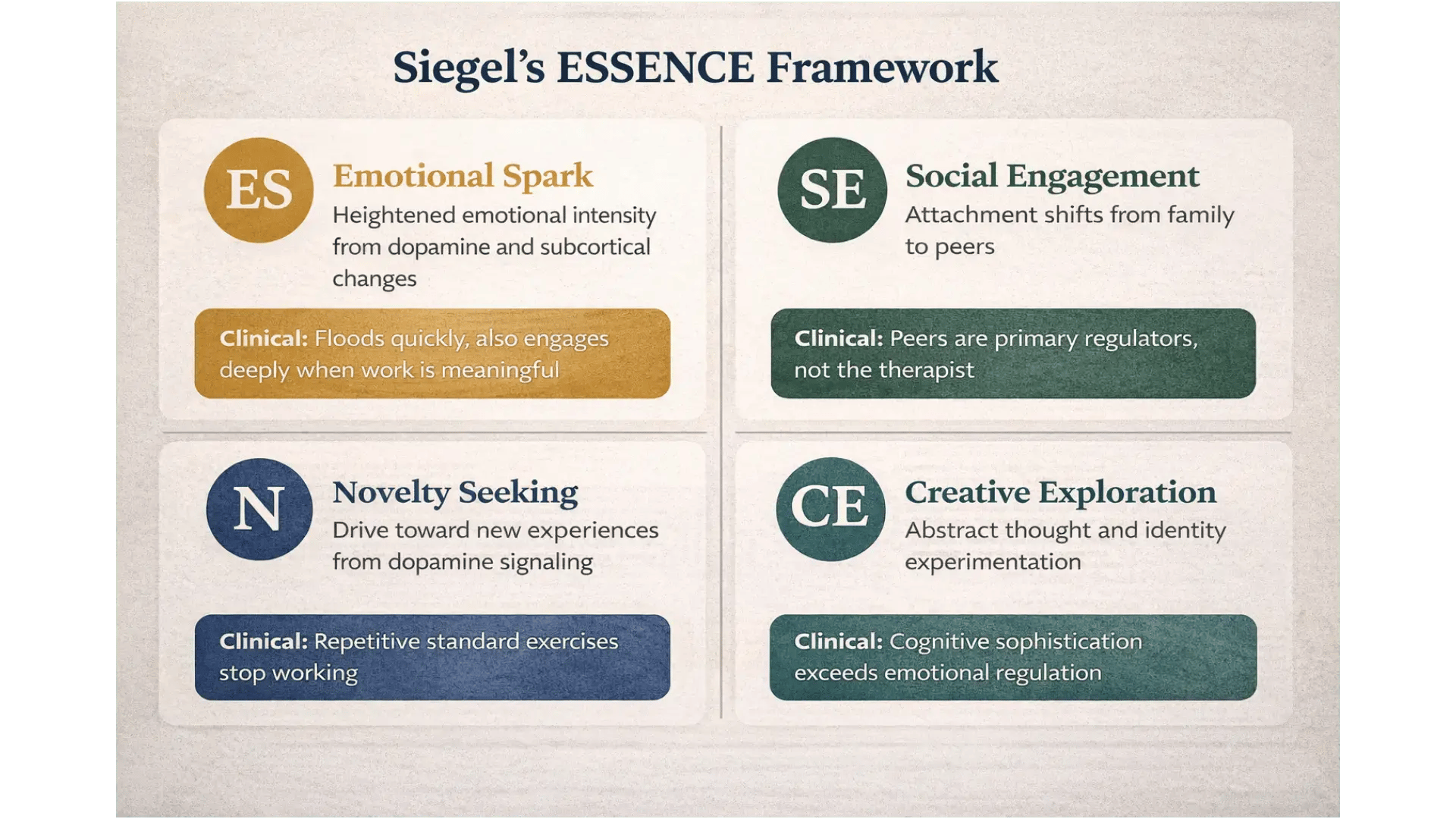
Emotional Spark describes the heightened emotional intensity that comes from changes in subcortical activity and dopamine signaling during adolescence. The downside is what looks like volatility: storms, moodiness, reactivity. The upside is the passion and depth of feeling that allow teenagers to be moved, motivated, and engaged in ways adults often cannot match. In the therapy room, this means that the same nervous system that floods quickly is also one that can engage deeply when the work is meaningful. A clinician who pathologizes the spark will lose the teenager. One who works with it has access to a quality of engagement that is difficult to find with adult clients.
Social Engagement reflects the developmental shift in attachment from family to peers. Teenagers turn outward, looking for membership and meaning in the social groups they are forming. Clinically, this matters because the therapist is not the teenager’s primary source of relational regulation. Peers are. The therapy relationship still matters, sometimes profoundly, but it sits inside a larger relational context the clinician needs to understand and respect.
Novelty Seeking is the developmental drive toward new experiences, fueled by lower baseline dopamine and higher dopamine release in response to novelty. This is what gets teenagers out of the family of origin and into the world. It is also what makes the standard, repetitive structure of adult therapy feel deadening to a teenage brain. A teenager who has done the same safe place exercise three weeks in a row is not being resistant when she stops engaging with it. Her brain is correctly registering that it is not working.
Creative Exploration is the capacity for abstract thought, identity experimentation, and challenge to established frameworks. The downside is the questioning of everything, including the therapy itself. The upside is that adolescents can grasp clinical concepts and make symbolic connections in ways that genuinely surprise clinicians who underestimate them. The cognitive sophistication is real, even when the emotional regulation has not caught up to it.
Each of these features is at odds with how adult-facing therapy is usually structured. The clinician who understands ESSENCE works with these qualities rather than against them.
The teenage brain was built to do its remodeling under conditions of relative safety. When trauma is part of the picture, particularly chronic, developmental, or relational trauma, the remodeling process itself is disrupted in ways that single-incident adult trauma rarely produces.
Research on neurobiological development in the context of childhood trauma documents specific structural and functional changes in stress-sensitive regions including the hippocampus, the prefrontal cortex, and the amygdala (Pechtel & Pizzagalli, 2011; reviewed in McCrory et al., 2017). Sustained activation of the HPA axis, the body’s primary stress response system, can interfere with neurotrophic gene expression and protein synthesis in the very regions the adolescent brain is supposed to be refining. The result is reduced neurogenesis, altered connectivity, and degraded communication between regions that are still developmentally working out their relationships to each other.
The clinical translation is that complex trauma in adolescence does not simply produce trauma symptoms. It produces trauma symptoms layered onto a brain whose architecture has been shaped by the very stress it is trying to process. A comprehensive review of the biological effects of childhood trauma showed that maltreated children who experienced trauma across multiple developmental periods had more externalizing and internalizing problems and lower IQ scores than children maltreated in only one period, suggesting that trauma duration has cumulative cognitive effects (De Bellis & Zisk, 2014). For an EMDR clinician, this means that an adolescent with complex trauma is rarely presenting with one clean target memory. She is presenting with a developmentally shaped system that has been trying to function under chronic stress, often for years.
Single-incident trauma in an adolescent looks different. A car accident, an assault, a single overwhelming event in an otherwise relatively stable system tends to produce a cleaner clinical picture: discrete intrusive symptoms, a recognizable target memory, more contained dysregulation. Standard EMDR adapted for adolescents often moves through this kind of presentation efficiently. Complex trauma, in contrast, requires preparation that addresses the developmental system as a whole, not just the discrete memory. The two presentations are not the same kind of clinical problem.
The Adaptive Information Processing model that underlies EMDR proposes that the brain has an innate capacity to process experience and integrate it into adaptive memory networks. When this processing system is overwhelmed, memories are stored in a state-specific, fragmented form, disconnected from the broader networks that would normally give them context and meaning (Hase et al., 2017). EMDR works, in the AIP framework, by activating these dysfunctionally stored memories and facilitating their reconsolidation into adaptive networks.
The model holds for adolescents, but the developmental specifics matter. The networks into which memories are supposed to integrate are themselves still under construction. When a teenager experiences trauma during the remodeling period, the memory is not just isolated from existing adaptive networks. It is laid down in a system whose adaptive networks are not fully formed.
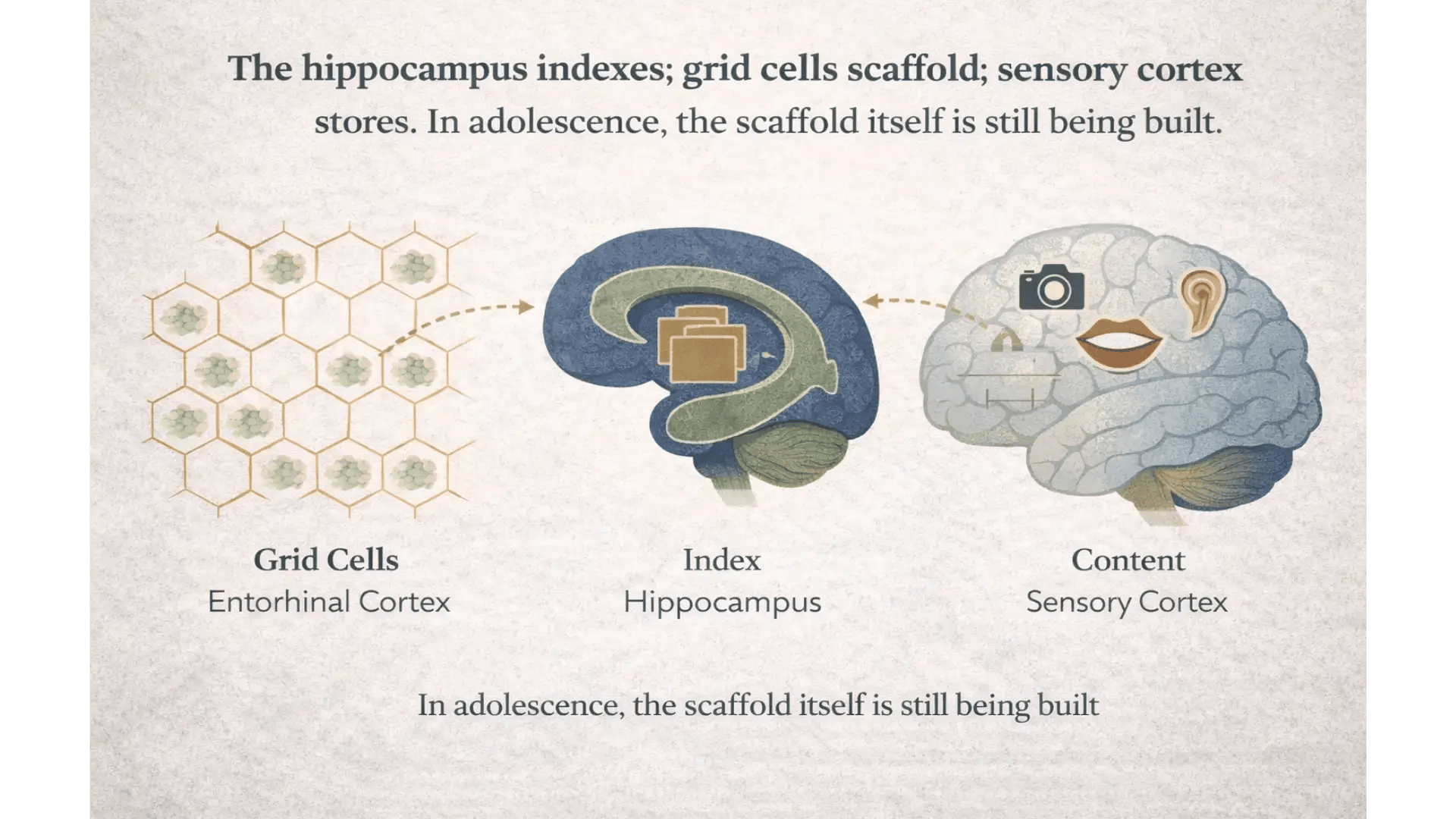
Recent computational neuroscience offers a useful refinement here. The Vector-HaSH model, published in Nature in 2025, proposes that the hippocampus and entorhinal cortex together create a high-capacity memory system using grid cells as a structured scaffold (Chandra et al., 2025). Memories are not stored in the hippocampus directly. The hippocampus functions more like an index, with grid cells creating a spatial scaffolding that points to where content is stored in sensory cortex. This framework is congruent with the AIP model. It also offers a specific account of why adolescent trauma memories may be stored differently than adult ones: the scaffold itself is still being built.
For target generation in adolescent EMDR, the implications are practical. Memory networks in teenagers are often less consolidated, less verbal, and more sensory than in adults. A target may not yet have a clear narrative; it may live as a body sensation, an image, an affect state, or a relational pattern that cannot quite be put into words. The clinician who waits for an adolescent to produce an adult-style target description is often waiting for something the developing brain is not yet capable of producing in that form. Adapting how targets are identified, how they are accessed, and how they are processed is not a deviation from AIP fidelity. It is fidelity to the model applied to a developmental brain.
Several clinical decisions look different when neurodevelopment is held in mind throughout the work.
Pacing changes. Phase 2 preparation with adolescents typically takes longer than the protocol-only timeline suggests, particularly with complex trauma presentations. The work is not just to install resources but to build, alongside the resources, enough internal scaffolding for processing to land somewhere. With adults, the adaptive networks that processing draws on are often already there. With teenagers, they may be partially in place at best.
Preparation changes. The standard SUD scale, the standard safe place visualization, the standard guided imagery: each of these was developed for adult cognition and adult tolerance for performative inner work. Adolescents often need concrete, sensory, and spatially organized resources, like the Safe/Calm Estate Jon Roberts teaches. They also benefit from preparation that uses the spatial scaffolding their brains are already employing for memory: imagined spaces with rooms, video game environments, real physical locations.
Processing changes. Working memory is still developing through ages thirteen to fifteen, with strategic self-organization not reaching adult levels until sixteen or seventeen. Standard ninety-minute reprocessing with sustained dual attention is, for many teenagers, beyond capacity. Shortened processing exposures of fifteen to twenty minutes, with built-in containment breaks, protect against the flooding and shutdown that derail teen sessions. Titration techniques that constrict the processing field, like EMD or EMDr, are often more appropriate than full standard processing.
Target selection changes. Targets in adolescent work are more likely to be implicit, sensory, or relational than in adult work. A teen may not be able to articulate the memory at all in standard cognition-emotion-body-sensation format, but she may be able to draw it, point to where she feels it, or name a song or a video game scene that captures it. These are not workarounds. They are appropriate adaptations for a brain that stores experience differently than an adult brain does.
Closure and integration change. Phase 7 closure, including the use of the imagined estate or other developmentally appropriate containment, becomes more important rather than less. The same is true for Phase 8 reevaluation, which often reveals that what looked like consolidation in one session has shifted by the next. Teen brains are still doing work between sessions in ways adult brains are not.
Do teenagers process trauma differently than adults? Yes, in several specific ways. Adolescent memory networks are still being consolidated, working memory is still maturing, and the prefrontal regulation that supports dual attention during processing is not fully online until the late teens or early twenties. Trauma in adolescence is also more likely to interact with developmental processes themselves, particularly with chronic or complex presentations. EMDR works with adolescents when these differences are accounted for in pacing, preparation, and processing technique. It often does not work, or destabilizes, when the adult protocol is applied unchanged.
What is the best therapy for teenage trauma? The honest answer is that it depends on the presentation, the teen, and the clinician. For PTSD in adolescents, EMDR has accumulating evidence as an effective treatment, including in complex PTSD presentations when adapted appropriately. Trauma-focused cognitive behavioral therapy (TF-CBT) also has strong evidence. The more useful question is whether the clinician working with a particular teen has the developmental knowledge and clinical skill to adapt their chosen modality to the brain in the room. Modality fidelity without developmental adaptation is often where treatment breaks down.
Can adolescents handle EMDR if they have complex or developmental trauma? Many can, and many benefit substantially from it, when the work is adapted for complex presentations: longer preparation, parts-informed assessment, modified processing, attention to dissociation and high-risk behaviors, and developmentally appropriate language and structure throughout. The adaptation is the discipline. Without it, complex adolescent EMDR is one of the harder ways to make a teen worse.
The clinician who internalizes adolescent neurodevelopment makes different choices in real time. She does not push through a teen’s apparent verbal articulation when the body is telling a different story. She does not treat a stalled session as a clinical failure when the working memory in the room may have simply maxed out. She does not interpret a teenager’s resistance to a guided imagery exercise as resistance to therapy when it is more accurately a brain that has correctly identified a developmental mismatch. She does not assume that what looks like a clean target is actually clean; she assumes there are sensory and relational layers that the teen has not yet found language for.
None of this is mystical. It is the application of available developmental neuroscience to clinical decision-making that already happens in every session. The clinician is going to make those decisions either way. The question is whether she is making them with the developing brain in mind or without it.
For clinicians who want to deepen this work, having a structured framework for adolescent EMDR, one that integrates neurodevelopment, parts work, modified preparation, and processing adaptations, is what turns scattered clinical instinct into a discipline that can be taught, practiced, and improved across cases. That framework exists. It is what separates clinicians who dread teen clients from clinicians who have found something rigorous and meaningful in the work.
EMDR with Adolescents: Parts Work, Modified Processing, and High-Risk Behaviors is a five-module on-demand training with Jon Roberts, LCSW, CAS. Module 1 covers the neurobiology of the adolescent brain in clinical depth, with the rest of the course showing you how that neuroscience translates into preparation, parts work, modified processing, and protocols for high-risk behaviors. 5 CEs (EMDRIA, ASWB ACE, NBCC). Available July 30, 2026.
I’m Ready to Work More Effectively With Teen Clients →
References
Chandra, S., Sharma, S., Chaudhuri, R., & Fiete, I. (2025). Episodic and associative memory from spatial scaffolds in the hippocampus. Nature, 638, 739-751. https://www.nature.com/articles/s41586-024-08392-y
De Bellis, M. D., & Zisk, A. (2014). The biological effects of childhood trauma. Child and Adolescent Psychiatric Clinics of North America, 23(2), 185-222. https://pmc.ncbi.nlm.nih.gov/articles/PMC3968319/
Hase, M., Balmaceda, U. M., Ostacoli, L., Liebermann, P., & Hofmann, A. (2017). The AIP model of EMDR therapy and pathogenic memories. Frontiers in Psychology, 8, 1578. https://pmc.ncbi.nlm.nih.gov/articles/PMC5613256/
McCrory, E. J., Gerin, M. I., & Viding, E. (2017). Annual research review: Childhood maltreatment, latent vulnerability and the shift to preventative psychiatry. Journal of Child Psychology and Psychiatry, 58(4), 338-357. https://pmc.ncbi.nlm.nih.gov/articles/PMC6428430/
Murty, V. P., Calabro, F., & Luna, B. (2016). The role of experience in adolescent cognitive development: Integration of executive, memory, and mesolimbic systems. Neuroscience & Biobehavioral Reviews, 70, 46-58. https://pmc.ncbi.nlm.nih.gov/articles/PMC5074888/
Siegel, D. J. (2014). Brainstorm: The power and purpose of the teenage brain. Tarcher. https://drdansiegel.com/the-essence-of-adolescence/
