
When Eating Disorders Meet EMDR: Rethinking 'Symptoms' as Survival Strategies
Feb 27, 2026
Written By: Susan Yuen, LMFT
Read Time: 10 Minutes
I remember sitting in my first EMDR training, scribbling notes about targeting traumatic memories, watching the instructor demonstrate bilateral stimulation with such confidence. The model was elegant. The protocol was clear. And nowhere in those three days did anyone mention what to do when the "symptom" keeping your client alive is an eating disorder.
Years later, after my own journey through disordered eating and decades of working with complex trauma, I've learned this: eating disorders and disordered eating aren't symptoms to eliminate. They're responses to overwhelming experiences, chronic shame, disrupted attachment, and nervous system dysregulation. They're survival strategies that made perfect sense at the time they were developed, even if they're causing harm now.
My goal in creating this EMDR training for eating disorders is to help EMDR clinicians conceptualize eating disorders and disordered eating within trauma and attachment networks, not as pathology to fix, but as adaptive responses to understand, honor, and eventually help clients outgrow when they're ready.
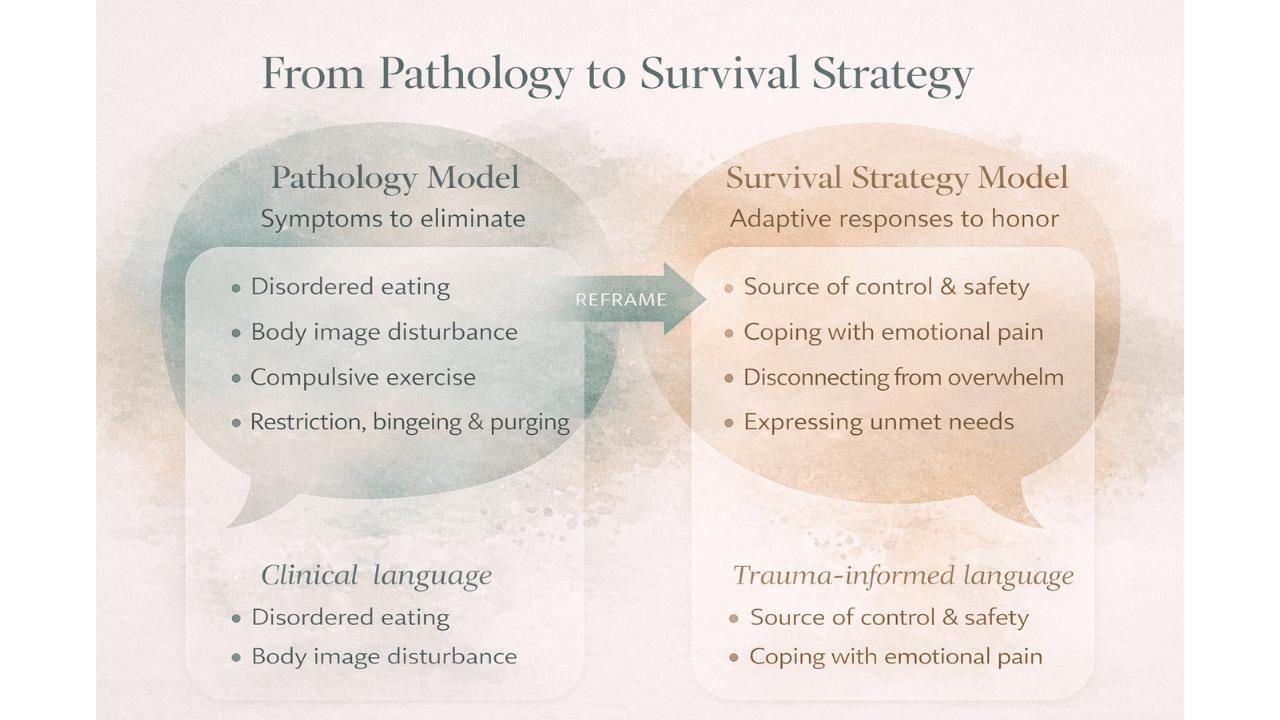
Beyond Pathology: Why "Symptom" Language Falls Short
Here's what bothers me about how we've been trained to talk about eating disorders: we use the language of symptoms, severity scales, and diagnostic criteria as if we're describing a broken system that needs repair. But what if the system isn't broken? What if it's working exactly as designed, protecting someone from something unbearable?
When we reframe eating disorders and disordered eating from pathology to adaptive survival response, everything shifts. Restriction becomes a way to control the uncontrollable. Bingeing becomes self-soothing when nothing else feels safe. Purging becomes a release valve for shame that has nowhere else to go. Orthorexia becomes moral certainty in a world that feels morally chaotic.
This isn't just semantics. The way we conceptualize these behaviors changes how we assess readiness, plan treatment, and show up in the therapy room. Research on trauma and eating disorders consistently shows that trauma histories are significantly overrepresented in eating disorder populations. But standard treatment often focuses on symptom management, meal plans, cognitive restructuring, exposure hierarchies, without addressing the underlying trauma networks driving the behaviors.
Moving beyond symptom management toward trauma-informed, liberation-centered work means asking different questions. Not "How do we stop this behavior?" but "What is this behavior protecting? What would happen if this strategy disappeared tomorrow? What else needs to be in place first?"
That's the clinical stance this training is built on.
ED Behaviors Inside Trauma and Attachment Networks
Let me paint you a picture from my own practice. I worked with a client whose restrictive eating began at age twelve, right after her youth pastor praised her for "finally looking more modest" after she'd lost weight during a stomach flu. The memory wasn't about food. It was about belonging, worthiness, and the message that her body's visibility was something shameful that needed to be controlled.
Attachment theory research on eating disorders shows what many of us see clinically: eating disorder behaviors often develop in response to attachment injury, performance pressure, powerlessness, and environments where love feels conditional. When you grow up in a high-control religious environment where your body is surveilled and judged, restriction can feel like spiritual devotion. When you're told repeatedly that your worth is tied to appearance, eating disorders become a logical response to an impossible standard.
Through an EMDR lens, these behaviors aren't random symptoms. They're solutions embedded in memory and attachment networks. The memory network linking food restriction to worthiness, thinness to safety, control to love, these are the networks we need to target. But we can't target them effectively if we're only seeing "anorexia nervosa" instead of seeing the adaptive strategy that made sense given everything this person survived.
Here's what this looks like in EMDR case conceptualization:
Past: The shaming comment from a parent. The racist beauty standard was internalized by the media. The sexual abuse where the body felt like a target. The religious message that hunger is virtue and appetite is sin.
Present: The trigger that activates restriction today. The relationship dynamic that brings up bingeing. The body-based cue that spirals into compensatory exercise.
Future: What identity, safety, and belonging look like beyond the eating disorder.
When you map eating disorder behaviors into these trauma and attachment networks, you're not treating a symptom. You're addressing the memories and relational patterns that created the need for the symptom in the first place.
Survival Strategies in the Body: Control, Numbing, and Belonging
Let's talk about what these survival strategies actually do for people.
Control in chaos or rigidity: I've worked with clients who grew up in homes where everything felt unpredictable, violence, substance use, financial instability. Food became the one thing they could control. I've also worked with clients who grew up in rigidly controlled environments, religious fundamentalism, authoritarian parenting, perfectionist pressure, where eating disorder behaviors became the only form of rebellion or the ultimate expression of obedience.
Numbing unbearable affect: For clients with trauma histories, bingeing can function the same way substances do, creating a state change that makes overwhelming emotions temporarily tolerable. Restriction can do the same thing, numbing through deprivation rather than excess. Studies on trauma-related eating disorders show that these behaviors often serve emotion regulation functions in the absence of other coping skills.
Belonging through conformity: Here's where weight stigma, diet culture, racism, and gendered harm come in. We live in a culture that equates thinness with worthiness, discipline, and moral superiority. For women, for people in larger bodies, for people of color navigating racist beauty standards, for anyone whose body has been surveilled and judged, eating disorder behaviors can feel like the price of admission to belonging.
Research on weight stigma experiences documents the profound psychological harm of weight-based discrimination. When a client tells me they started restricting after being told they'd "let themselves go," I'm not hearing vanity. I'm hearing a survival response to a culture that punishes certain bodies.
This is why EMDR training for eating disorders needs to explicitly address psychosocial, cultural, and systemic contributors. These aren't background factors. They're the soil these survival strategies grow in.
Mapping ED Survival Strategies with Parts and Attachment Lenses
One of the most powerful tools I use in EMDR case conceptualization with eating disorders is parts-informed mapping. When you start identifying the different parts carrying eating disorder behaviors, you can see exactly what each part is trying to accomplish.
The perfectionistic part that drives orthorexia or exercise compulsion, trying to earn worthiness through performance.
The controlling part that manages restriction, creating safety through predictability and structure.
The numbing part that uses bingeing or purging to escape unbearable affect or dissociation.
The parentified part that learned early on to make themselves small, quiet, and undemanding to keep the peace.
Each of these parts is linked to specific memories. The perfectionistic part might be carrying the memory of a parent's disappointment. The controlling part might be holding the terror of chaos or abuse. The numbing part might be protecting from body shame messages internalized from racist or gendered beauty standards, medical stigma, or religious purity culture.
When you map these parts to their origin memories, you have your EMDR target plan. But here's the critical piece: you can't target these memories effectively if you're trying to eliminate the part doing the protecting. You have to build internal cooperation first.
This means Phase 2 work that helps different parts communicate, understand each other's protective intentions, and eventually trust that there are other ways to meet the needs the eating disorder has been meeting. It means using EMDR with an attachment lens that honors how these behaviors developed in relational contexts and will likely shift in relational contexts too.

What This Reframe Changes in EMDR Assessment and Readiness
When you shift from "stop the symptom" to "what is this protecting?", your entire assessment process changes.
Instead of asking "How severe is the eating disorder?" you're asking:
- How central is this strategy to the client's sense of safety and control right now?
- What would collapse if this behavior disappeared tomorrow?
- What other regulation resources does this person have?
- How much do they understand about the protective function of their eating disorder behaviors?
This is where readiness assessment gets nuanced. A client whose eating disorder is their only way to manage overwhelming affect probably needs more Phase 2 stabilization work before reprocessing. A client whose medical instability is severe might need a higher level of care before outpatient EMDR is appropriate.
But here's what I want you to understand: readiness isn't about waiting for the eating disorder to resolve before you can do trauma work. It's about building enough nervous system regulation, relational support, and internal cooperation that the client can afford to start letting go of the survival strategy.
Research on EMDR therapy for eating disorders emphasizes the importance of thorough stabilization before moving into reprocessing. This isn't just best practice. It's what keeps clients safe when you're asking them to revisit the very experiences that made the eating disorder necessary in the first place.
Planning EMDR When Survival Strategies Are Still Active
So how do you actually do EMDR with clients whose eating disorder behaviors are still very active?
First, you honor the protective intention. You don't go into session with an agenda to eliminate restriction or stop bingeing. You go in with curiosity about what these behaviors are protecting and a commitment to building other options before you threaten the only coping strategy someone has.
This means robust Phase 2 work:
- Polyvagal-informed regulation that helps clients reconnect with body signals in a way that feels safe, not activating.
- Compassion-focused resourcing that addresses the shame and self-criticism woven through eating disorder presentations.
- Parts work that maps the internal system and builds communication between parts before you ask them to change.
When you do move toward targeting memories, start with the foundation, not the eating disorder behavior itself. Target the shame experiences. The attachment injuries. The messages about unworthiness. The memories where someone learned their body was wrong, too much, not enough, or inherently shameful.
Let me give you an example. Instead of targeting "the first time I binged," you might target "the comment my father made about my body when I was nine." Instead of targeting "my fear of gaining weight," you might target "the message I learned in youth group that my body was a stumbling block to men."
When you process the memories feeding the survival strategy, the strategy itself often shifts organically. Clients don't need to be convinced to let go of eating disorder behaviors. They need the underlying trauma and attachment injuries to heal so the behaviors become unnecessary.
This is clinical nuance you don't get in standard EMDR training. It's what specialized EMDR training for therapists treating eating disorders is designed to teach.
How Specialized EMDR Training Supports This Reframe
Let me be transparent about why I created this training. After two decades of doing EMDR with eating disorder and disordered eating clients, I kept seeing the same gaps in standard EMDR education:
- Limited guidance on identifying the adaptive functions of eating disorder behaviors within memory networks.
- Minimal training on readiness assessment specific to medical instability and eating disorder presentations.
- Almost no discussion of how to integrate weight stigma, diet culture, and systemic oppression into EMDR case conceptualization.
- Insufficient attention to protocol selection—when to use DeTUR versus FSAP versus standard protocol with eating disorder clients.
This training addresses those gaps directly. You'll learn:
- Assessment and case conceptualization that maps eating disorder behaviors into trauma and attachment networks, identifying protective parts and their origin memories.
- Phase 2 stabilization tailored to eating disorder presentations, including regulation strategies that don't inadvertently trigger eating disorder behaviors and resourcing that addresses body shame and perfectionism.
- Readiness criteria that go beyond symptom severity to evaluate nervous system stability, relational support, and whether the eating disorder is currently the primary survival strategy.
- Protocol selection and interweaves designed specifically for eating disorder themes like control, worthiness, body safety, and identity beyond performance.
- Relapse prevention using EMDR approaches like DeTUR to address urges and triggers in a way that honors the protective intention while building alternative responses.
The curriculum integrates current research on EMDR and trauma-related eating disorders with practical, immediately applicable clinical skills. It's not theoretical. It's what you need to do this work safely and effectively in outpatient or private practice settings.
Inviting a Different Question: "What Is This Behavior Protecting?"
Here's the question I want you to carry into every session with a client struggling with eating disorder or disordered eating behaviors:
What is this behavior protecting?
Not "What's wrong with this client?" or "How do I make this stop?" but "What is this behavior protecting, and how do I honor that while helping the client build other options?"
This question shifts the entire therapeutic stance from pathologizing to curious, from combative to collaborative. It aligns with the liberation-centered, shame-attuned approach that defines both my clinical work and this training.
When you see eating disorders as survival strategies rather than symptoms, you're not just changing language. You're changing how you assess risk, plan treatment, pace processing, and show up in a relationship with your clients. You're moving from a medical model that sees "disordered eating" to a trauma-informed model that sees adaptive responses to overwhelming circumstances.
And honestly? Your clients will feel the difference. They'll feel seen instead of pathologized. They'll feel understood instead of judged. And they'll be more likely to trust you enough to eventually let go of the survival strategies that have kept them alive.
If this reframe resonates with you, if you're ready to deepen your understanding of EMDR for eating disorders and learn how to integrate this survival-strategy lens into your work, I'd love to have you join me in this training.

Ready to rethink how you conceptualize eating disorders in EMDR?
Join me for EMDR Training for Eating Disorders at the Trauma Therapist Institute. This is a live, online training offering 6 CEs, designed specifically for EMDR-trained clinicians who want to work more effectively with eating disorders and disordered eating presentations in outpatient settings.
You'll learn readiness assessment, case conceptualization, Phase 2 stabilization, protocol selection, and how to integrate weight stigma, diet culture, and systemic oppression into your EMDR work. Plus, you'll receive Dissociation Demystified as a bonus resource.
Because your clients with eating disorders deserve trauma-informed EMDR therapy. And you deserve the training that helps you offer it with confidence, competence, and deep respect for the survival strategies that brought them this far.
References
Beer, R. (2018). Protocol for EMDR therapy in the treatment of eating disorders. In Eye movement desensitization and reprocessing (EMDR) therapy scripted protocols and summary sheets. https://doi.org/10.1891/9780826194725.0001
Breland, J. Y., Donalson, R., Dinh, J. V., & Maguen, S. (2018). Trauma exposure and disordered eating: A qualitative study. Women & Health, 58(2), 160–174. https://doi.org/10.1080/03630242.2017.1282398
EMDR for Eating Disorders. (2026). Trauma Therapist Institute. https://www.traumatherapistinstitute.com/EMDR-for-Eating-Disorders-Assessment-Conceptualization-and-Intervention
Gerend, M. A., Lu, A. W., & Teets, E. L. (2025). Weight stigma and mental health in a racially and ethnically diverse sample of US adults. Frontiers in Psychiatry, 16, 1593145. https://doi.org/10.3389/fpsyt.2025.1593145
[email protected]. (2024, June 29). Trauma and eating disorders. National Alliance for Eating Disorders. https://www.allianceforeatingdisorders.com/trauma-and-eating-disorders/
Pellegrini, R. A., Finzi, S., Veglia, F., & Di Fini, G. (2021). Narrative and bodily identity in eating disorders: Toward an integrated theoretical-clinical approach. Frontiers in Psychology, 12, 785004. https://doi.org/10.3389/fpsyg.2021.785004
Schlapp, M. (2025, April 15). When trauma & eating disorders collide. National Eating Disorders Association. https://www.nationaleatingdisorders.org/trauma-and-eating-disorders-healing/
Team. (2022, June 17). Attachment theory and eating disorders. Attachment Project. https://www.attachmentproject.com/blog/attachment-theory-and-eating-disorders/
Trauma Therapy & EMDR Training | Trauma Therapist Institute. (2017). Trauma Therapist Institute. https://www.traumatherapistinstitute.com
Stay connected with fun info, news, promotions and updates!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.




